Positive Sagittal Balance and Management Strategies in Adult Spinal Deformities
Volume 1 | Issue 1 | Apr – June 2016 | Page 33-38|Charanjit Singh Dhillon1
Authors :Charanjit Singh Dhillon[1]
[1] MIOT Center for Spine Surgery, MIOT International, Chennai
Address of Correspondence
Dr Charanjit Singh Dhillon. MS, DNB, FNB Spine, D-Ortho,
Director MIOT Center for Spine Surgery, MIOT International, Chennai. India
Email: drdhillonc@hotmail.com
Abstract
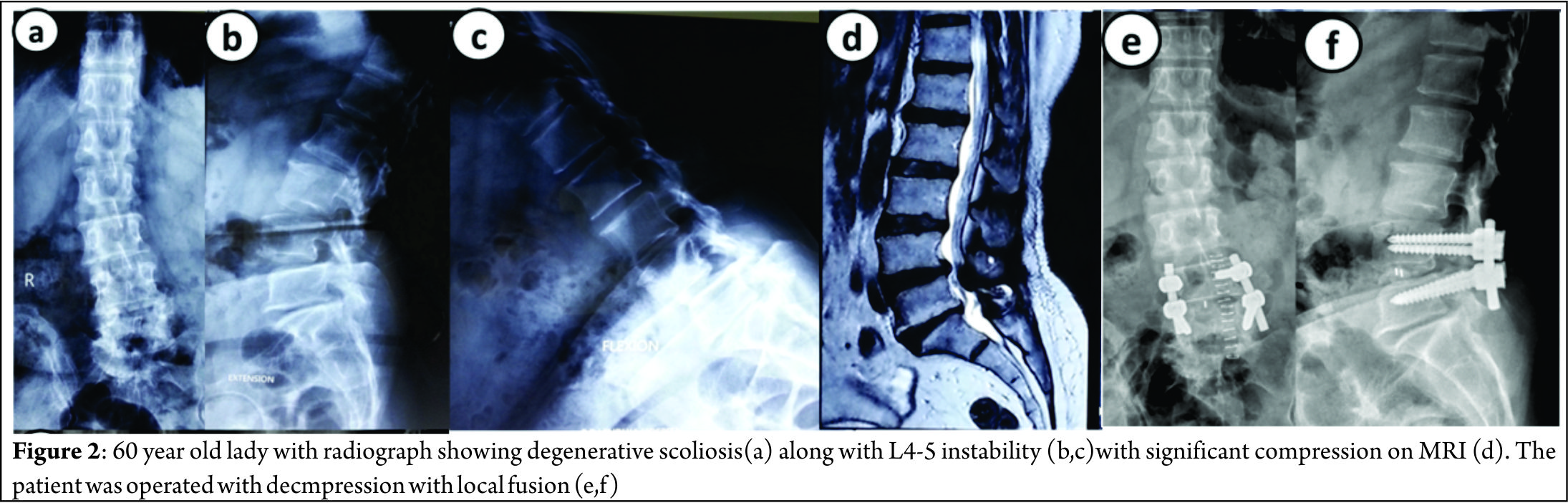
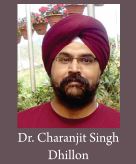
Human Spine has adapted a curved morphology to compensate for the upright posture. Normally these curves are sagittally balanced and a vertical line drawn from the center of the C7 vertebral body (the C7 plumb line) passes within a few millimeters of the posterior-superior corner of S1. A positive sagittal balance occurs when the C7 plumb line falls anterior to the posterior-superior corner of the S1 endplate. The extent of imbalance is measured as centimeters of deviation of the C7 plumb line (also known as Sagittal vertical axis- SVA) from the posterior-superior corner of the S1 endplate[4](Figure 2). Negative sagittal balance is much less common in clinical practice and rarely warrants surgical attention. In this article we shall deal with only positive sagittal balance which is encountered more often. The article covers the diagnosis and also details of surgical management. In absence of effective conservative measures, the patient seeking surgical remedies are on rise. Selecting the appropriate surgical technique to achieve spinal balance is crucial to success.
Keywords: Positive Sagittal Balance, Smith-Petersen Osteotomy, Pedicle Subtraction Osteotomy, Vertebral Column Resection
Introduction
Ever since man has assumed an erect posture and bipedal gait, a series of morphological changes have taken place in the homosapien vertebral column to adapt to this new challenge of upright posture. One of the most distinctive adaptive changes seen in human spinal column has been the assumption of a gentle ‘S’ curve in sagittal plane with thoracic kyphosis [TK] interposed between cervical and lumbar lordosis [LL]. These curves work like a coiled spring to absorb shock, maintain an upright balance and allow the spine to withstand great amounts of stress than what a straight column would otherwise absorb. At the same time it still allows for a wide range of movements in the cervical and the lumbar region to optimize the use of extremities while still maintaining an upright stance with the head centered over the pelvis and finally over both feet. In most individuals with a disease free and deformity free sagittally balanced spine, a vertical line drawn from the center of the C7 vertebral body (the C7 plumb line) passes within a few millimeters of the posterior-superior corner of S1[1] (Fig. 1).
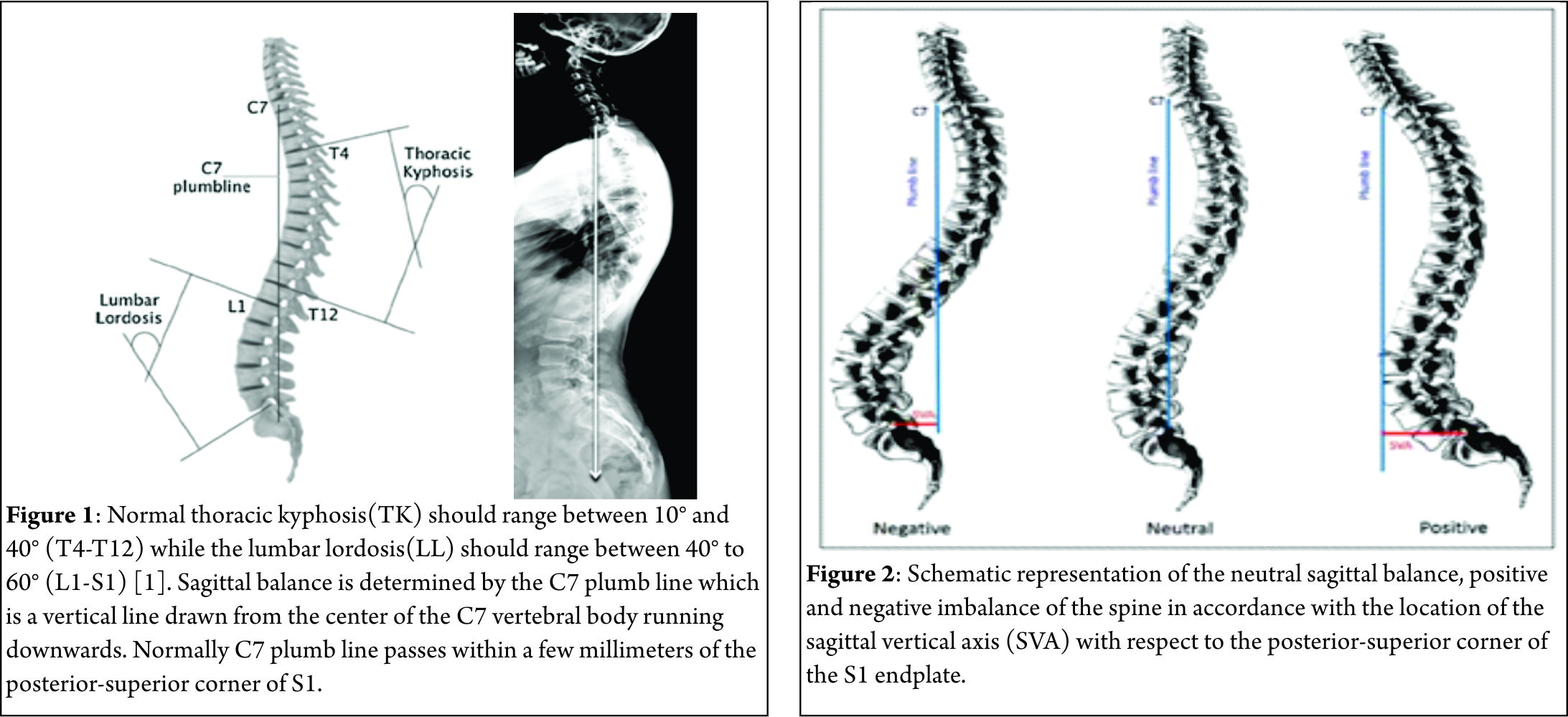
This is the most ergonomically favorable position for the spine to maintain an erect posture in the most energy-efficient manner. However, with progressively larger deviations from this ideal position, the endeavor to remain upright increases exponentially, thereby warranting greater muscular effort and energy to maintain standing balance[2]. By convention, positive sagittal balance occurs when the C7 plumb line falls anterior to the posterior-superior corner of the S1 endplate. Conversely, negative sagittal balance occurs when the C7 plumb line falls posterior to this point[3]. The extent of imbalance is measured as centimeters of deviation of the C7 plumb line (also known as Sagittal vertical axis- SVA) from the posterior-superior corner of the S1 endplate[4](Fig. 2). Negative sagittal balance is much less common in clinical practice and rarely warrants surgical attention. In this article we shall deal with only positive sagittal balance which is encountered more often.
Causes
Positive sagittal imbalance can occur due to destruction of the vertebral body by trauma, tumor or infection. It may also result from loss of LL as a consequence of multilevel degenerative disc disease, ankylosing spondylitis, diffuse idiopathic skeletal hyperostosis or osteoporosis[5]. Secondary causes include iatrogenic flat back syndrome resulting from failure of restoration of the appropriate LL according to the patient’s Pelvic incidence[PI]. Rarely, sagittal imbalance may be seen following spinal fusion surgery through an area of pseudarthrosis or through a degenerated segment adjacent to a previous fusion. In the past the use of distraction instrumentations such as the Harrington rods was the frequent cause of iatrogenic flat back syndrome[6]. Positive sagittal imbalance due to congenital deformities is outside the preview of this symposium on adult deformities.
Compensation
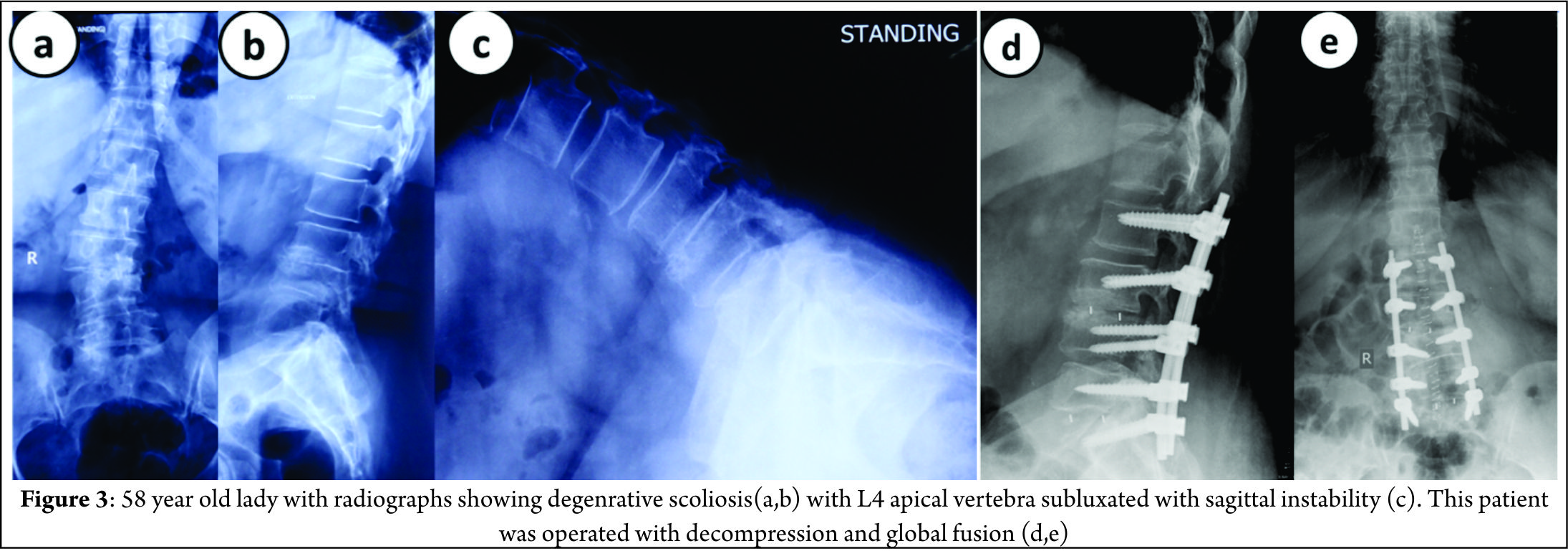
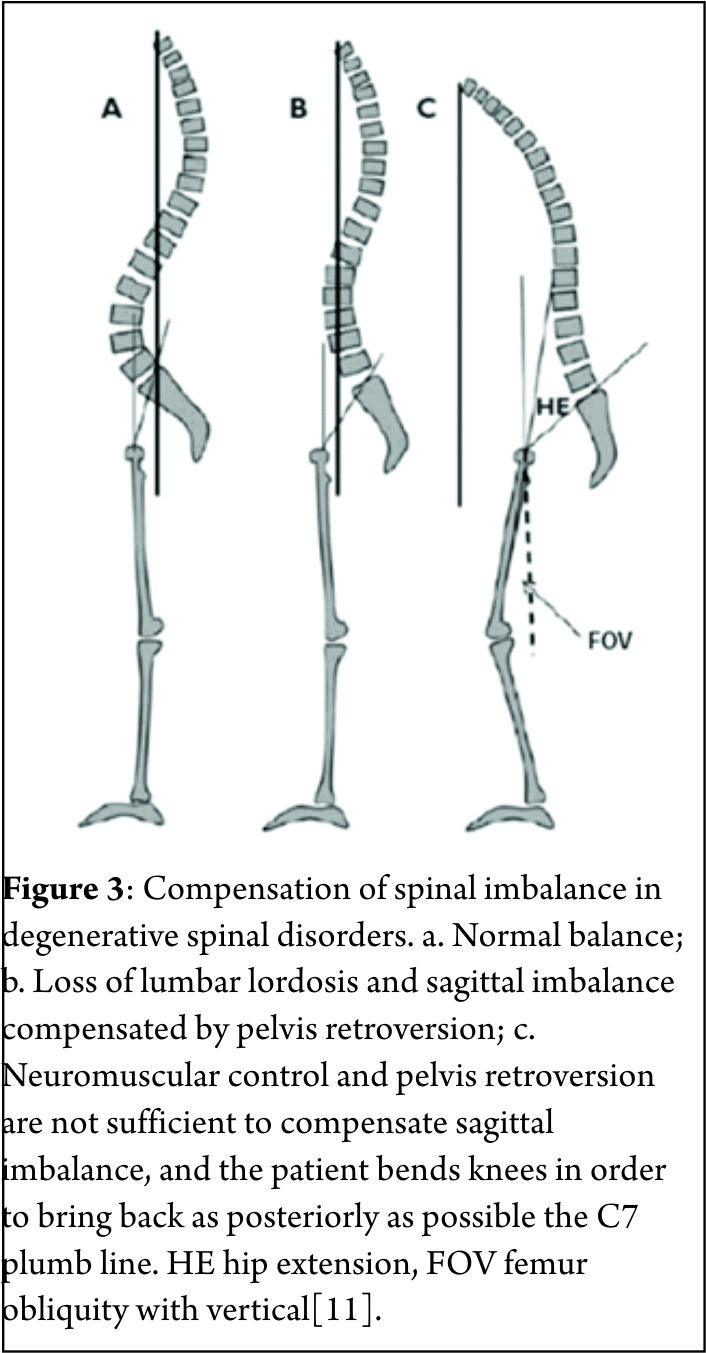
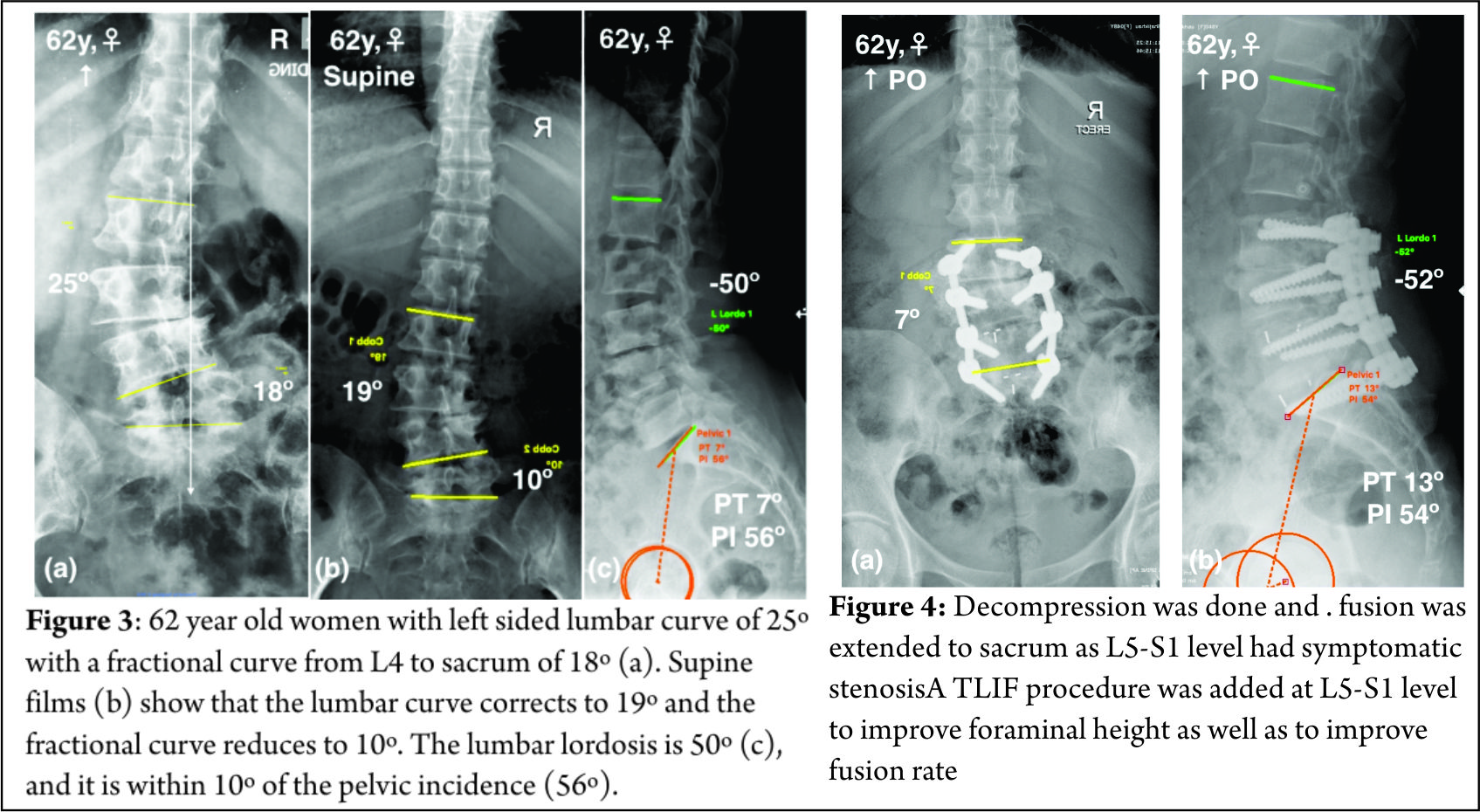
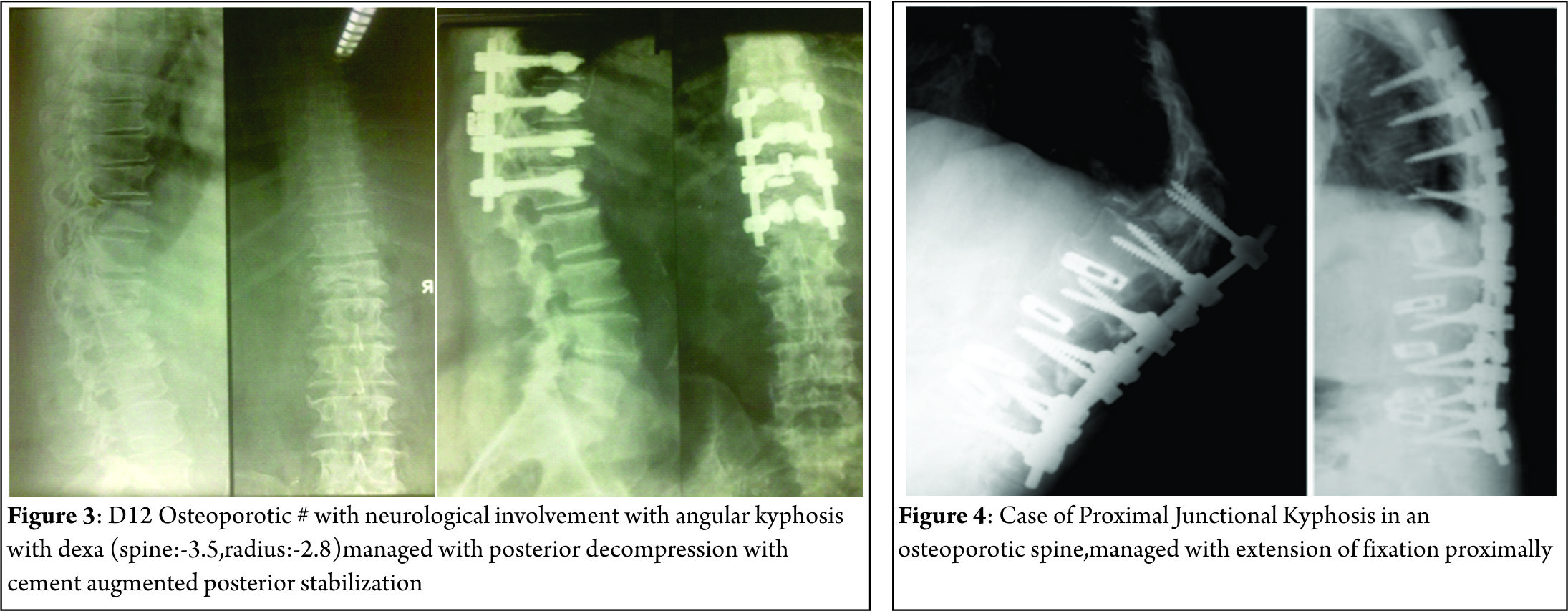
Barrey et al. [7] described three stages of compensatory mechanisms corresponding to the severity of the sagittal imbalance: balanced, balanced with compensatory mechanisms and imbalanced spine. In the initial stages when positive sagittal imbalance begins, the pelvis retroversion takes place in an attempt to push the C7 plumb line backwards behind the femoral heads resulting in extension of the hips[7-9]. At this stage the PI determines the global capacity of pelvis retroversion and consequent compensatory capability. In patients with higher PI the pelvis can tilt more and compensate better than patients with a low PI[10]. The full body is now balanced but it is a compensated balance, which is less efficient[11]. At the same time the posterior spinal muscles act as a posterior tension band (trying to restore some LL) pulling the adjacent segments of the lower dorsal spine into hyperextension. In young patients with flexible spines this hyperextension leads to reduction of TK. Spine hyperextension is an energy consuming process that generates increase of stresses on posterior structures resulting in risk of retrolisthesis, facet joints overstress and even sometimes isthmic lysis (Fig. 3) [11]. When pelvis retroversion and spine hyperextension are not enough to keep the C7 plumb line behind the femoral heads, the only solution to keep the gravity line between the two feet is to bend the knees. This process needs good psoas and quadriceps muscles activity, which is again energy consuming and not an efficient situation. When the knee flexion also fails to keep the C7 plumb line behind the femoral heads, a stage of decompensation (imbalance) is reached and an external aid (e.g., crutches, walker) is often required to maintain upright posture[11].
Imaging Studies
Standard full-length anteroposterior and lateral radiographs should be performed in all patients with suspected sagittal imbalance. Horton et al[12] reported the ‘clavicle position’ in which the patient stands with both hips and knees fully extended, the elbows fully flexed, the wrists flexed with the hands in a relaxed fist placed into the supraclavicular fossa without any external support as the best patient position for the study of sagittal deformity. Sagittal imbalance is basically determined by the C7 plumb line offset from the posterior-superior corner of S1 (Fig. 2). An offset >2.5 cm anteriorly or posteriorly is considered to be abnormal[13]. Different components such as TK, LL and PI are also measured to define the overall sagittal balance[14]. Dynamic lateral radiographs with the spine in full flexion and full extension helps to assess the mobility of discs in the kyphotic segment and hence plan appropriate surgical management. Alternately, some surgeons use traction views to assess spine mobility.
Management
Nonsurgical Management
Symptomatic patients with sagittal imbalance are often unresponsive to nonsurgical treatment. Physical therapy programs, bracing, facet joint injections, selective nerve root blocks and epidural steroid injections[15] are often ineffective in decompensated patients.
Surgical Management
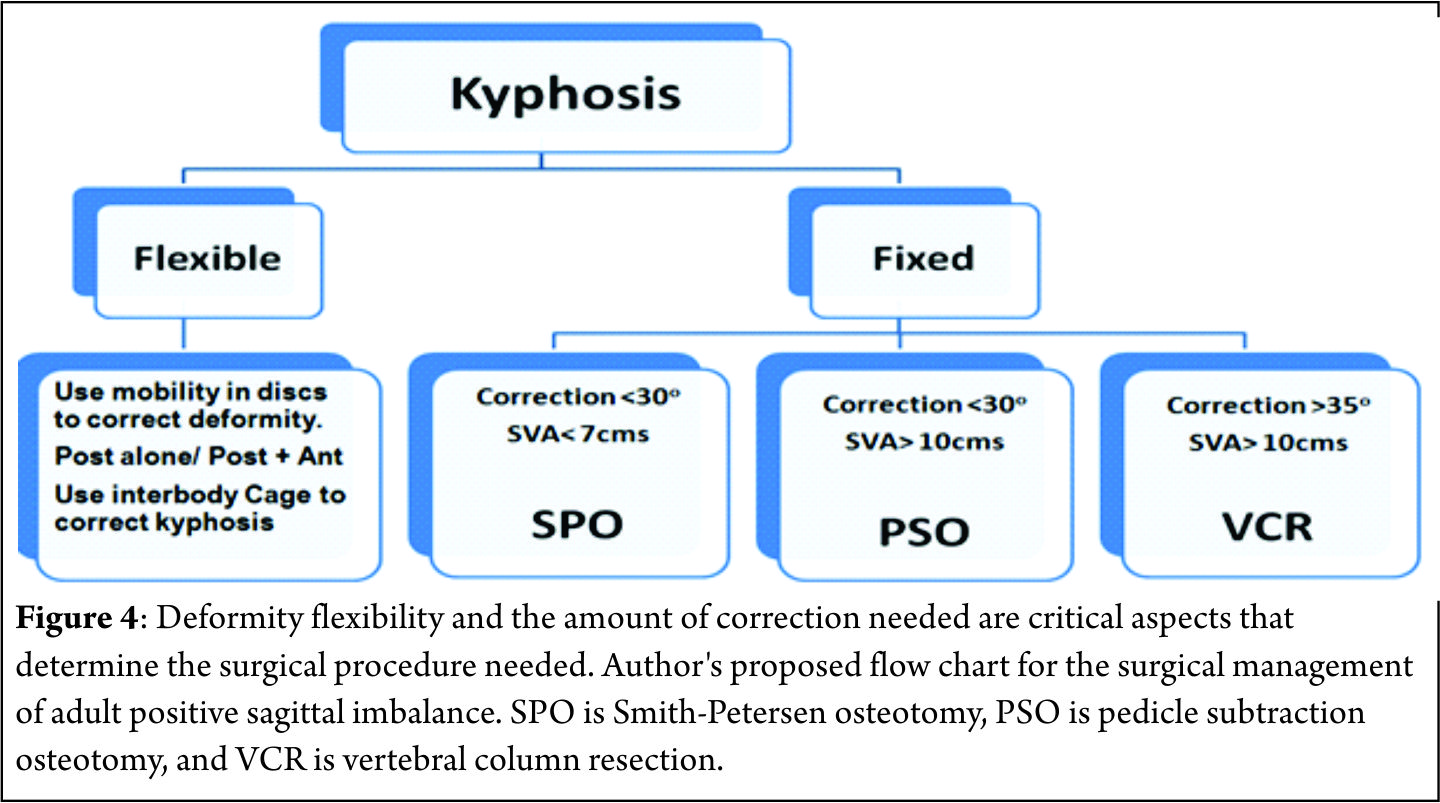
Surgery is the mainstay of treatment for patients with sagittal deformity[15]. Indications include failure of nonsurgical treatment, kyphosis progression, significant back pain, radicular symptoms and exhaustion due to effort to maintain upright stance. The goals of surgery are to achieve a solid fusion with a balanced spine in both sagittal and coronal planes, relieve pain, and prevent progression of imbalance. Several studies have shown that adequate restoration of sagittal plane alignment is necessary to significantly improve clinical outcome and avoid pseudarthrosis[16,17]. Prior to surgery, the patient should be evaluated for risk factors such as pulmonary and cardiac disease, osteoporosis, smoking, and malnutrition. Careful consideration should be given to especially elderly patients due to higher incidence of pseudarthrosis and complications[17,18]. Relative contraindications to major spinal reconstructive surgery include psychiatric disease, uncontrolled diabetes, osteoporosis, substantial cardiopulmonary disease, and poor family or social support[19]. Flexibility of the spine should be assessed radiologically using long-cassette standing and supine AP and lateral radiographs and lateral dynamic flexion and extension radiographs. Patients’ standing sagittal imbalance may decrease in supine or prone position due to mobile segments. Bridwell[20] classified spinal deformities into three categories based on curve flexibility: totally flexible, partially flexible through mobile segments, and fixed deformity with no correction in the recumbent position. Flexible deformities can be addressed with anterior-posterior or posterior only surgery not requiring any osteotomy[6]. Sagittal balance is improved by lengthening the anterior column, either through an anterior or a posterior approach, using cages, structural allograft or autograft. The posterior column is then shortened with laminectomies (when there is evidence of stenosis), facetectomies and fusion with compression instrumentation to correct kyphosis. Fixed deformities can be managed by anterior-only, combined anterior and posterior or posterior-only approaches. Spinal osteotomies like the Smith-Petersen osteotomy[SPO], pedicle subtraction osteotomy [PSO], and vertebral column resection[VCR] are often employed to correct the stiff apical kyphotic segment. The amount of correction needed determines the type of osteotomy warranted (Fig. 4). With recent advances in instrumentation and techniques, posterior-only approaches have become more popular. Numerous studies support the safety and efficacy of a posterior-only approach for the treatment of most spinal deformities[21,22]. Fusion across the L5-S1 junction is mandatory in the presence of lumbosacral pathology, such as postlaminectomy defects, lumbar spinal stenosis, oblique take-off of L5, and L5-S1 disc degeneration to reduce the risk of pseudoathrosis and loss of fixation[22].
Smith-Petersen Osteotomy [SPO]
In 1945, Smith-Petersen and associates[23] were the first to describe a posterior osteotomy for correction of fixed sagittal deformity in patients with rheumatoid arthritis. In 1946, La Chapelle[24] described a modification of Smith-Petersen’s technique by adding an anterior release in a case of ankylosing spondylitis. The use of this osteotomy for the treatment of flat back deformity was first reported by Moe and Denis in 1977[25]. In 1984 Ponte[26] described multiple chevron osteotomies with spinal instrumentation in a patient with Scheuermann’s disease.
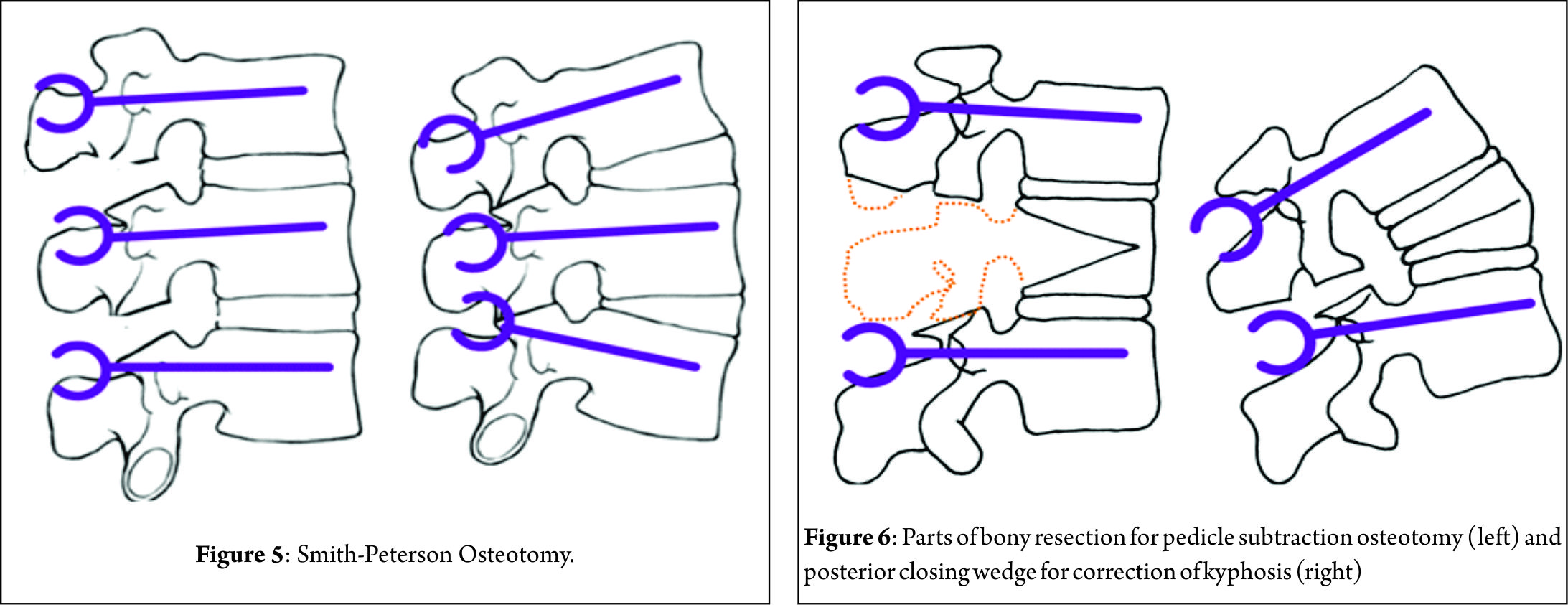
The surgical technique involves removal of all the posterior ligaments (supraspinous, interspinous, and ligamentum flavum) and facets to produce a posterior release. Dissection is then performed laterally to decompress the nerve roots. The lamina is beveled to allow sufficient room for the dura and nerve roots after closure of the osteotomy. The osteotomy hinges at the posterior border of the vertebral body and creates hyperextension by closing the posterior elements and opening the anterior elements providing sagittal plane realignment. Posterior segmental pedicle screw instrumentation is used to maintain closure of the osteotomy (Fig. 5). It should be emphasized that either a mobile disc or an anterior release is required to allow lengthening of the anterior column.
The SPO should be considered for patients with C7 plumb line that is less than 7 cm positive[27]. Amount of correction provided by a single SPO is in the range of 4-10° depending on the disc height and the mobility of the disc. One degree of correction is usually achieved per millimeter of bone resected posteriorly[27]. The SPO is technically easier and safer than other osteotomies offering a reduction in operative time, blood loss and risk of neurological complications, although rupture of the great vessels has been reported following anterior-column lengthening in an unfortunate case[23].For the patient requiring 10° to 20° of lordosis or 6-8 cm of correction of the C7 plumb line, it is more appropriate to perform multiple SPOs than one PSO, unless the fixed deformity is fused anteriorly[27].
Pedicle-Subtraction osteotomy [PSO]
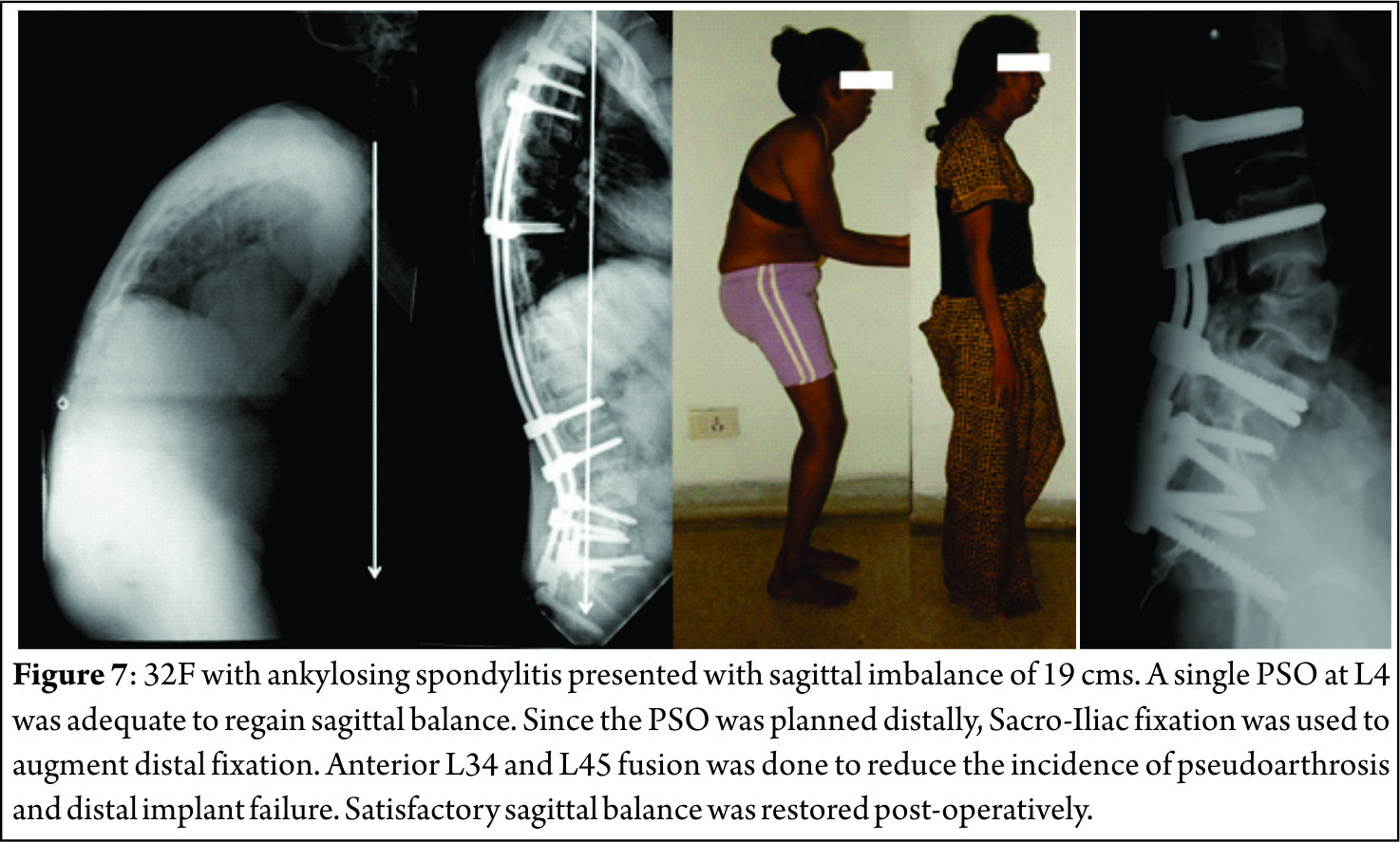
In 1963, Scudese and Calabro[28] were the first to describe a monosegmental intravertebral closing wedge posterior osteotomy of the lumbar spine. Later, Thomasen[29] reported on 11 patients with ankylosing spondylitis treated with posterior closing wedge osteotomies. In the same year, Heining et al[30] described an eggshell osteotomy as a variant of the PSO. The PSO is performed by removing the posterior elements and both pedicles, performing a transpedicular V shaped wedge osteotomy of the vertebral body, and closing the osteotomy by hinging on the anterior cortex (Fig. 6) achieving bone-on-bone contact in the posterior, middle, and anterior columns[31]. Central canal enlargement is critical to avoid neurologic injury during closure of the osteotomy. Posterior segmental pedicle screw instrumentation is used to maintain the correction. Instrumentation of at least three vertebral levels above and below the osteotomy is recommended[32]. The PSO has the advantage of obtaining correction through all the three spinal columns, while the posterior and middle columns shorten, this osteotomy does not lengthen the anterior column avoiding stretch on the major vessels and viscera anterior to the spine[33]. An average of 30º to 40º correction can be achieved with one level PSO[34]. The ideal candidates for a PSO are patients with a fixed sagittal imbalance of more than 10 cm and those patients who have circumferential fusion along multiple segments, which would contradict multiple SPOs(Fig. 7)[27].
Although PSOs are more technically demanding and more prone to complications than SPOs, PSOs provide satisfactory clinical and radiologic outcomes in long-term follow-up. Kim et al[34] in a series of 35 PSOs reported their good results with 87% patient satisfaction and 69% restoration of function after more than 5 years of follow-up. Cho et al[35] compared one level of PSO with three levels of SPOs in their study and reported that an average total kyphosis correction was 31.7º for PSO group and the improvement in the sagittal imbalance (11.2 ± 7.2 cm) was much better than multiple SPOs. Blood loss was significantly higher in PSO group but there was no statistical difference between one level PSO and three levels of SPO groups with respect to operating times. Regarding neurological complications, Buchowski et al[36] reported a postoperative immediate neurological deficit rate of 11.1% which subsequently reduced to 2.8% during follow up. Deficits were mostly unilateral and never proximal to osteotomy site, often did not correspond to the level of osteotomy, and surprisingly were not detected by neuromonitoring[36].
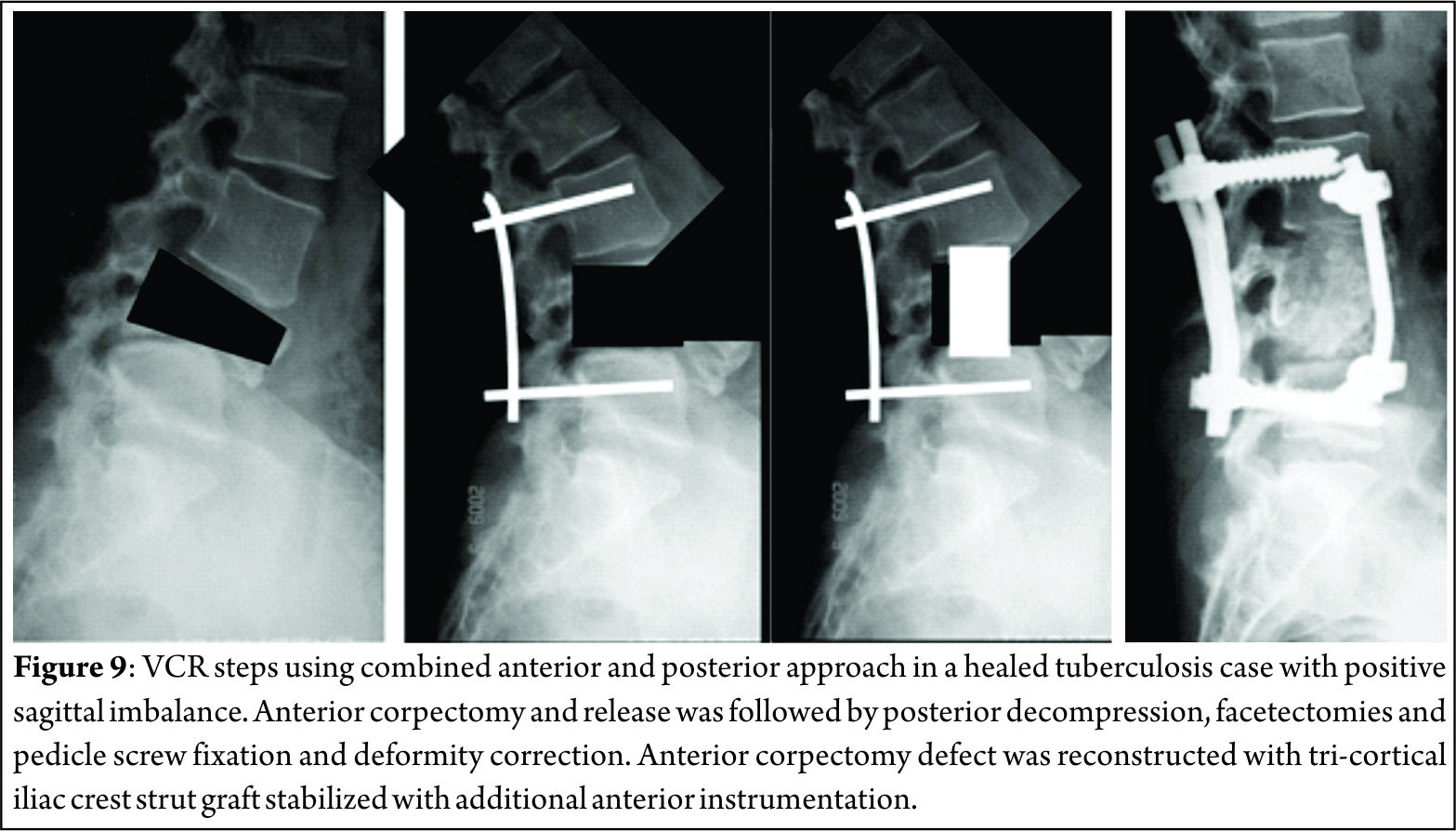
Vertebral Column Resection [VCR]
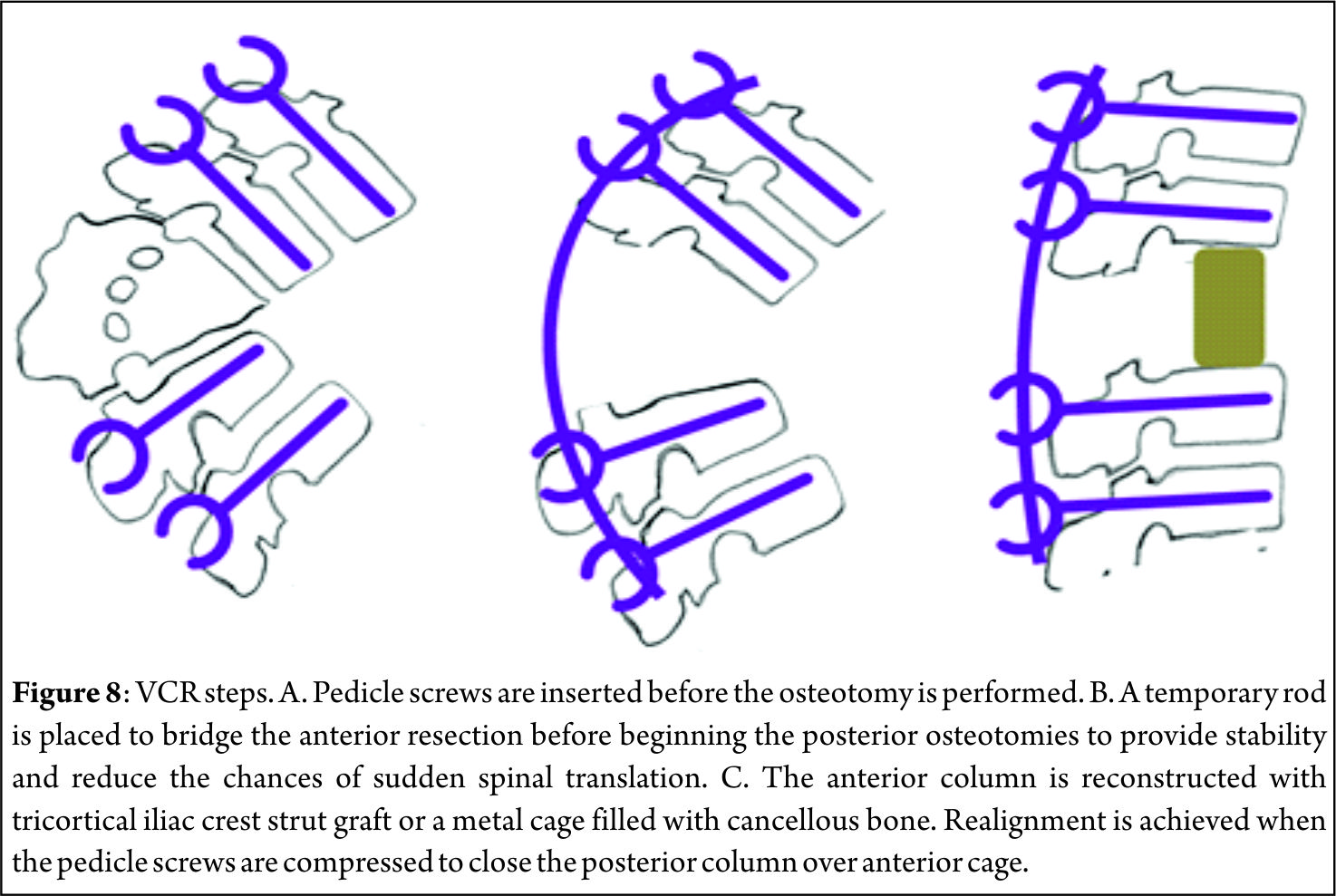
VCR was first described in 1922 by MacLennan[37] as a combined anterior and posterior procedure and was popularized by Bradford and Tribus[38] as a method of correcting severe coronal deformity and combined coronal and sagittal deformity. It is indicated in rigid severe deformities of the spine such as congenital kyphosis, rigid multiplanar deformities, sharp angulated deformities, posttraumatic deformities and spondyloptosis. The VCR technique is a challenging procedure involving the complete resection of the posterior elements and the vertebral body including adjacent discs of one or more levels (Fig. 8) providing controlled manipulation of both the anterior and posterior columns simultaneously. It can be performed using either combined anterior and posterior approaches or a posterior-only approach[39]. Of all the spinal osteotomies, VCR provides the greatest amount of correction. Suk et al[40] reported a correction of 61.9o in the coronal plane and 45.2o in the sagittal plane in their series of 70 patients after VCR. In their series of 35 patients, Lenke[41] reported major curve improvements of 55o in global kyphosis cases, 58o in angular kyphosis cases and 54o in kyphoscoliosis cases after VCR. Vertebral column resection through a posterior-only [PVCR] approach has become popular in the recent years. Suk[40] and Lenke[41] popularized the use of PVCR for severe deformities of the spinal column. PVCR enables simultaneous manipulation and control of both anterior and posterior spinal columns and thus provides better correction than other types of osteotomies. It is a single procedure compared to combined anterior and posterior VCR, reducing the total operating time and the amount of blood loss and also avoiding opening of the thoracic cage and pleura. Avoiding anterior surgery may be very beneficial for patients with severe pulmonary function compromise because of severe thoracic deformity[27]. Inspite of all advantages, PVCR is a technically demanding procedure. One major concern with PVCR is the potential for neurologic complications, which may result from direct neurologic injury during bone resection or deformity correction. Neurologic complications may also result from subluxation of the spinal column, dural buckling and compression of the spinal cord by residual bone or soft tissues in the canal after correction[27]. Suk[40] reported a 34.3% overall rate of complications and a 17.1% rate of neurological complications. Lenke[41] reported a similar 40% overall rate of complications and an 11.4% rate for neurological complications. Hamzaoglu[39] reported neurological complications of 7.84%.
Conclusions
With rising life expectancy the number of patients seeking consultation for pain due to sagittal imbalance is increasing. In the absence of effective conservative measures, the patient seeking surgical remedies are on rise. Selecting the appropriate surgical technique to achieve spinal balance is crucial to success. SPO, PSO and VCR all play an important role in the armamentarium of the spine deformity surgeon. However, each of these procedures are technically demanding and carries a certain amount of risks. Appropriate preoperative optimization of the patient as well as preoperative surgical planning are critical in order to avoid potential complications. Surgical achievement of the ideal spinopelvic alignment parameters is the desired goal. Nevertheless, even a partial improvement in these parameters is very likely to translate into substantial clinical benefits.
References
1 Bernhardt M, Bridwell KH. Segmental analysis of the sagittal plane alignment of the normal thoracic and lumbar spines and thoracolumbar junction. Spine 1989; 14: 717-721
2 Dubousset J. Three-dimensional analysis of the scoliotic deformity, in Weinstein SL (ed): The Pediatric Spine: Principles and Practice. New York, NY: Raven Press, 1994, pp 479-496.
3 Vedantam R, Lenke LG, Keeney JA, et al. Comparison of standing sagittal spinal alignment in asymptomatic adolescents and adults. Spine 1998; 23: 211-225
4 Gelb DE, Lenke LG, Bridwell KH, et al. An analysis of sagittal spinal alignment in 10° asymptomatic middle and older aged volunteers. Spine 1995; 20: 1351-1358.
5 Kim KT, Lee SH, Suk KS, Lee JH, Im YJ. Spinal pseudarthrosis in advanced ankylosing spondylitis with sagittal plane deformity: Clinical characteristics and outcome analysis. Spine 2007; 32: 1641-1647
6 Bridwell KH, Lenke LG, Lewis SJ. Treatment of spinal stenosis and fixed sagittal imbalance. Clin Orthop Relat Res 2001; 384: 35-44
7 Barrey C, Jund J, Noseda O, Roussouly P. Sagittal balance of the pelvis-spine complex and lumbar degenerative diseases. A com-parative study about 85 cases. Eur Spine J 2007; 16: 1459-1467
8 Barrey C, Jund J, Perrin G, Roussouly P. Spinopelvic alignment of patients with degenerative spondylolisthesis. Neurosurg 2007; 61: 981-986
9 Berthonnaud E, Dimnet J, Roussouly P, Labelle H. Analysis of the sagittal spine and pelvis using shape and orientation parameters. J Spinal Disord Tech 2005; 18: 40-47
10 Barrey C, Roussouly P, Perrin G, Le Huec JC. Sagittal balance disorders in severe degenerative spine. Can we identify the com-pensatory mechanisms? Eur Spine J 2011 Sep; 20 Suppl 5: 626-633
11 Le Huec JC, Charosky S, Barrey C, Rigal J, Aunoble S. Sagittal imbalance cascade for simple degenerative spine and consequenc¬es: algorithm of decision for appropriate treatment. Eur Spine J 2011 Sep; 20 Suppl 5: 699-703
12 Horton WC, Brown CW, Bridwell KH,Glassman SD, Suk SI, Cha CW. Is there an optimal patient stance for obtaining a lateral 36” radiograph? A critical comparison of three techniques. Spine 2005; 30: 427-433
13 Jackson RP, McManus AC. Radiographic analysis of sagittal plane alignment and balance in standing volunteers and patients with low back pain matched for age, sex, and size: A prospective con¬trolled clinical study. Spine 1994; 19: 1611-1618
14 Hammerberg EM, Wood KB. Sagittal profile of the elderly. J Spi¬nal Disord Tech 2003; 16: 44-50
15 Bradford DS, Tay BK, Hu SS. Adult scoliosis. Surgical indications, operative management, complications, and outcomes. Spine 1999; 24: 2617-2629
16 Bridwell KH, Lewis SJ, Lenke LG, Baldus C, Blanke K. Pedicle subtraction osteotomy for the treatment of fixed sagittal imbal¬ance. J Bone Joint Surg Am 2003; 85: 454-463
17 Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Pseudarthro¬sis in long adult spinal deformity instrumentation and fusion to the sacrum: Prevalence and risk factor analysis of 144 cases. Spine 2006; 31: 2329-2336
18 Booth KC, Bridwell KH, Lenke LG, Baldus CR, Blanke KM. Complications and predictive factors for the successful treatment of flatback deformity (fixed sagittal imbalance). Spine 1999; 24: 1712-1720
19 Hu SS, Berven SH. Preparing the adult deformity patient for spi¬nal surgery. Spine 2006; 31(19 suppl): S126-S131
20 Bridwell KH. Decision making regarding Smith-Petersen vs. pedicle subtraction osteotomy vs. verterbral column resection for spinal deformity. Spine 2006; 31(19 suppl): S171-S178
21 Pateder DB, Kebaish KM, Cascio BM, Neubaeur P, Matusz DM, Kostuik JP. Posterior only versus combined anterior and posterior approaches to lumbar scoliosis in adults: A radiographic analysis. Spine 2007; 32: 1551-1554
22 Tsuchiya K, Bridwell KH, Kuklo TR, Lenke LG, Baldus C. Mini¬mum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine 2006; 31: 303-308
23 Smith-Petersen MN, Larson CB, Aufranc OE. Osteotomy of the spine for correction of flexion deformity in rheumatoid arthritis. Clin Orthop Relat Res 1969; 66: 6-9
24 La Chapelle EH. Osteotomy of the lumbar spine for correction of kphosis in case of ankylosing spondtlitis. JBJS 1946; 28: 851-858
25 Moe JH, Denis F. Abstract: The iatrogenic loss of lumbar lordo¬sis. Orthopedic Transactions 1977; 1: 131
26 Ponte A, Vero B, Siccardi GL. Surgical treatment of Scheuer¬mann’s kyphosis. In: Winter RB (ed) Progress in spinal pathology: kyphosis. Aulo Gaggi 1984 Bologna, pp 75–80
27 Enercan M, Ozturk C, Kahraman S, Sarıer M, Hamzaoglu A, Ala¬nay A. Osteotomies/spinal column resections in adult deformity. Eur Spine J 2013 Mar; 22 Suppl 2: S254-64
28 Scudese VA, Calabro JJ. Vertebral wedge osteotomy for correction of rheumatoid (ankylosisng) spondylitis. JAMA 1963; 186:627-631
29 Thomasen E. Vertebral osteotomy for correction of kyphosis in ankylosing spondylitis. Clin Orthop Relat Res 1985 194: 142-152
30 Heining CA. Eggshell procedure. In: Luque ER (ed) Segmental spinal instrumentation. Thorofare, Slack, pp 221-230
31 Bridwell KH, Lewis SJ, Rinella A, Lenke LG, Baldus C, Blanke K: Pedicle subtraction osteotomy for the treatment of fixed sagit¬tal imbalance: Surgical technique. J Bone Joint Surg Am 2004; 86(suppl 1): 44-50
32 Kim KT, Lee SH, Suk KS, Lee JH, Im YJ. Spinal pseudarthrosis in advancedankylosing spondylitis with sagittal plane deformity: Clinical characteristics and outcome analysis. Spine 2007; 32: 1641-1647
33 Henry Halm. Pedicle subtraction osteotomy for correction of congenital scoliokyphosis. Eur Spine J 2011; 20:995–996
34 Kim JY, Bridwell KH, Lenke GL, Cheh GE, Baldus C. Results of lumbar pedicle substraction osteotomies of fixed sagittal im¬balance a minimum 5-year follow-up study. Spine 2007; 32(20): 2189-2197
35 Cho KJ, Bridwell KH, Lenke GL, Berra A, Baldus C. Comparison of Smith-Petersen versus pedicle substraction osteotomy for cor-rection of fixed sagittal imbalance. Spine 2005; 30(18): 2030-2037
36 Buchowski JM, Bridwell KH, Lenke LG, Kuhns CA, Lehman RA, Kim JY, Stewart D, Baldus C. Neurologic complications of lumbar pedicle subtraction osteotomy a 10-year assessment. Spine 2007; 32(20): 2245-2252
37 MacLennan A. Scoliosis. BMJ 1922; 2: 865-866
38 Bradford DS, Tribus CB. Vertebral column resection for the treat¬ment of rigid coronal decompensation. Spine 1997; 22: 1590-1599
39 Hamzaoglu A, Alanay A, Ozturk C, Sarier M, Karadereler S, Ganiyusufoglu K. Posterior vertebral column resection in severe spinal deformities. Spine 2011; 36(5): 340-344
40 Suk SI, Chung ER, Kim JH et al. Posterior vertebral column re¬section for severe rigid scoliosis. Spine 2005; 30(14): 1682-1687
41 Lenke LG, O’Leary PT, Bridwell KH, Sides BA, Koester LA, Blanke KM. Posterior vertebral column resection for severe pedi¬atric deformity: minimum two-year follow-up of thirty-five con¬secutive patients. Spine 2009; 34: 2213-2221.
| How to Cite this Article: Dhillon CS. Positive sagittal balance and management strategies in adult Spinal deformities. International Journal of Spine Apr – June 2016;2(1):33-38 . |








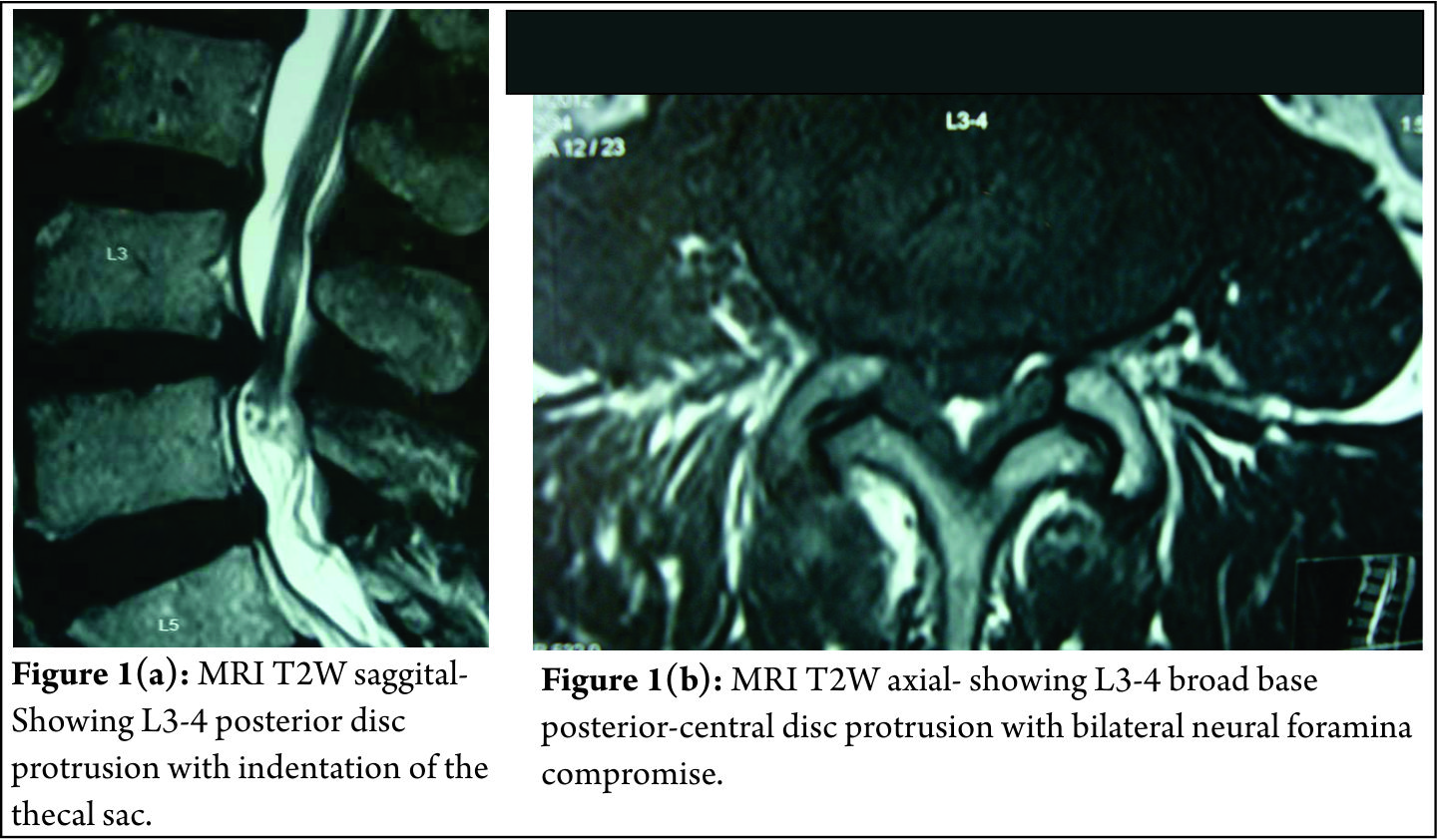
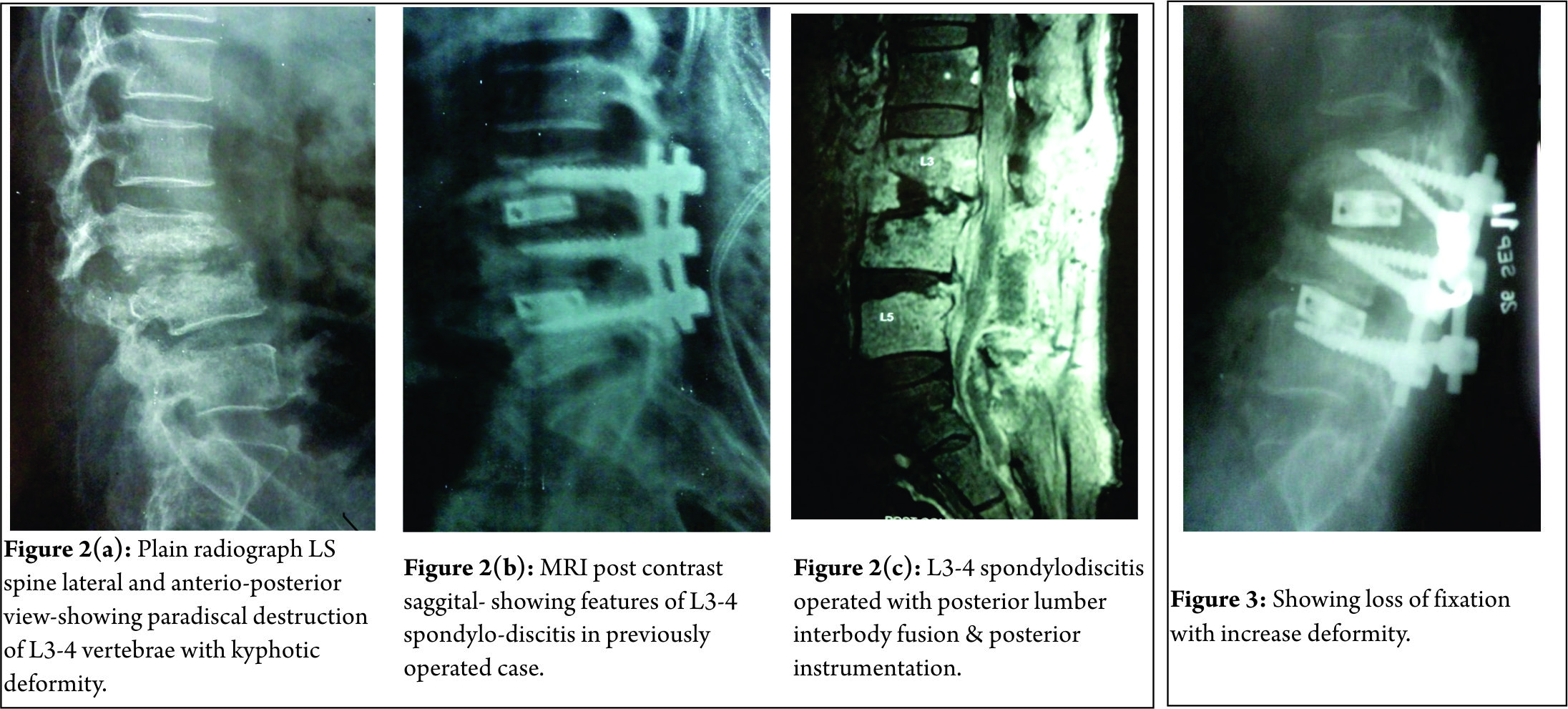
. MRI showed significant c ompression at l4-5 level (c). She was operated with decompression alone surgery")