Complications Encountered in Surgical Management Adult Spinal Deformities- Prevention and Management- A Retrospective Study in 193 Patients
Volume 1 | Issue 1 | Apr – June 2016 | Page 21-24|Hitesh N Modi[1], Bharat R Dave[1].
Authors :Hitesh N Modi[1], Bharat R Dave[1]
[1] Department of Spine Surgery, Zydus Hospital, Thaltej, Ahmedabad, GUJ and # Stavya Spine Hospital and Research Institute, Ellisbridge, Ahmedabad, GUJ.
Address of Correspondence
Dr. Hitesh N. Modi, Department of Spine Surgery, Zydus Hospital, SG highway, Thaltej, Ahmedabad, GUJ, INDIA. Email: modispine@gmail.com
Abstract
Background: Adult spinal deformity surgery is often associated with increased number of postoperative complications. Purpose of study was to elaborate encountered complications and possible ways to prevent and avoid such complications during surgery.
Methods: This was a retrospective analytical study in 193 patients with adult spinal deformity operated between 2010 and 2014 with decompression and multilevel pedicle screw fixation. Average age of patients was 64.5 years with minimum follow-up of 12 months. Clinical results were evaluated by excellent-good, fair and poor results on regular follow-up. Complications were elaborated in detail with possible causes and ways to prevent or avoid such complications to occur in future.
Results: There were 133 (69%) patients with excellent or good results while 35 (18%) patients with fair and 25 (13%) patients with poor results. There was 24.8% (n=48 out of 193) complication rate was found in the study. There were 20, 10, 6, 5, 3, 2, 1 and1 patients had persistent symptoms, respiratory difficulty, proximal junction kyphosis, dural puncture, deaths, wound infection, foot drop and renal failure, respectively. Reason for such complications were discussed in detail and precautions implemented in future surgeries.
Conclusion: There are higher postoperative complications rates noted in adult spinal deformity surgeries. Most common complications were proximal junctional kyphosis, respiratory difficulty and persistent symptoms postoperatively. Proper preoperative preparation and precautions to avoid such complications are necessary before surgical decision.
Key Words: Adult spinal deformity, surgical correction, postoperative complications, preventive measures.
Introduction
Surgeries, in earlier phase, were developed primarily to address and treat injuries or traumas causing death if not treated. Later on, as advances in surgeries progressed, it was focused to improve quality of life. Major advances in surgeries in recent era focused on overcome obstacles of bleeding, infection and pain as well as improved quality of life and earliest return to work without any disability [1]. Therefore surgical indications are found to be an elective application, including the complex conditions such as spinal deformity that typically affect quality of life rather than being an immediate threat to life. Adult spinal deformity is a significant problem for many patients affecting their quality of life, in particularly, the elderly people. India has around 100 million elderly at present and the number is expected to increase to 323 million, constituting 20 per cent of the total population, by 2050,” the report jointly brought out by United Nations Population Fund (UNFPA) and Help Age International said. Similarly in US also the number of elderly patients has been projected to increase to 19.6% from current 12.4% by the year 2030 [2]. Spinal deformity is a major morbidity in elderly population, with pain and balance problems associated with spinal deformity often representing a significant obstacle to mobility in this age group [3]. Nonsurgical management for adult or degenerative spinal deformity is likely underreported. While it is hypothesized that a majority of spinal deformity patients are treated non operatively by their primary physicians, and increasing number of patients are opting for surgery now days [4]. Adult deformity surgery in older patients is becoming an increasingly common and requested procedure. Average life expectancy is rising with an increased expectation for extended quality of life. However, despite improved technical capabilities, complications remain a common occurrence and a significant concern in adult deformity surgery. There are many literatures published showing favorable results with adult spinal deformity surgeries; however, actual prevalence of complications varies widely [5-9]. Several reports have reported a complication rate of greater than 40% in the literature. A meta-analysis published by Yadla et al, who reviewed 3299 patients, found a 41.2% complication rate [10]. In another multicenter retrospective series of 306 primary lumbar adult or degenerative scoliosis patients older than 50, Charosky et al have shown an overall complication rate of 39% [11]. Daubs et al, in their series of 46 complex adult deformity patients aged 60 years or older, presented a complication rate of 37% [12]. In patients older than 70, Lonergan et al reported 95% of patients experiencing a complication of some type [13]. It is also important to note that variety of complications reported in literature varies in terms of minor or major complication. The purpose of this article was to identify commonly associated complications encountered during adult or degenerative scoliosis surgery, to identify and elaborate the risk factors and methods to overcome and avoid such complications. In addition we aimed at literature review of such complications to educate about it to our patients prior to surgery.
Material and Methods
This is a retrospective analytical study of 193 patients operated for degenerative or adult spinal deformity between 2010 and 2014. Average age of patients was 64.5 (SD=10.5) years (Table 1).
TABLE 1
All patients were operated by both the authors. The indications of surgery were primarily chronic mechanical low back pain, radicular symptoms, lumbar stenosis and degenerative scoliosis. All patients were explained about possible outcome with extent of surgery as well as longer recovery time than the routine. Additionally all patients were put on calcium supplementation medications prior to the surgery. All patients were operated with pedicle screw fixation and posterolateral fusion along with decompression of affected lumbar spine and correction of spinal deformity to achieve sagittal balance. All surgeries were performed with open surgical technique with wide subperisteal exposure of all operative levels till the tips of transverse processes which was followed by free-hand pedicle screw instrumentation and attempting curve correction by facetectomy with rod derogation maneuver. Decompression laminectomy with or without discectomies were performed at the only affected levels with bilateral foramina decompression. Pedicure subtraction osteotomy was performed in only indicated patients where there was gross sagittal imbalance with kyphotic deformity noted. Postoperative follow-up was done at 6weeks, 3, 6, 12 months and yearly thereafter. There was follow-up of patients apart from protocol also if there is any complication or urgent assistance needed. Results were analyzed using relief in symptoms and improvement in quality of life as well as VAS score for pain. Results were divided in to excellent and good results that had postoperative recovery in their symptoms more than 80% and 60-80%, respectively. If patient had recovery in symptoms by 40-60% and less than 40%, there were categorized in to fair and poor results accordingly. Perioperative and postoperative complications were specifically recorded and studied in detail for this study. Complications that were recorded from operative period to three months postoperative period were included in perioperative complications [14]. Complications seen after three months were included in postoperative complications. Revisions after complications were also studied separately to identify the cause.
Results and Complications
Average follow-up was 24.1 months (SD= 9.1) with minimum follow-up 12 months. There were 28 patients having at least one level listless, 69 patients with two or less level severe stenosis, and rest 96 patients having problems at more than two levels along with degenerative scoliosis (Table 1).
TABLE 1
There were 5 patients with associated dorsolumbar stenosis (tendom stenosis), one with cervical myelopathy, one with intra-dural tumor, and eight with associated compression fractures and three with discitis apart from main pathology of stenosis or instability. All pathologies were addressed and operated along with correction of degenerative scoliosis and decompression of stenotic part or stabilization of instability. Evaluation of our results at the final follow-up shows that there were 133 (69%) patients with excellent or good results while 35 (18%) patients with fair and 25 (13%) patients with poor results (Table 2).
TABLE 2
Evaluating our complications (Table 2), there were three (who were included in poor results) deaths (1.5%); out of them one was due to pulmonary embolism and rest two were due to postoperative cardiac events. There was one patient from fair results who needed hemodialysis for acute renal shut down during perioperative period which recovered after 4 weeks with 21 cycles of hemodialysis. Six (3.1%) patients were having adjacent level degeneration or implant loosening causing myelopathy symptoms that required revision surgery (Fig 1-2).

On further evaluating them, all of them were having severe osteoporosis of bone marrow density for wrist and hip scan. All of them were kept of Teriperatide injections for at least one year and after that they did not have any further squeals. One patient had postoperative foot drop which recovered partially over a period of three months as implant positioning were found adequate on postoperative CT scan. This patient had having severely stenotic preoprerative canal size, and therefore, reason for foot drop was mainly due to handling of roots. There were five (2.6%) dural punctures during surgery which were repaired uneventfully. There were only two (1%) patients with postoperative wound infections; one with superficial and one with deep infections. Both were healed after debridement and appropriate antibiotics. Both patients were having positive urine culture due to prolonged catheterization postoperatively. There were 10 (5.2%) patients with postoperative oxygen saturation stays below 90% mainly due to pain and obesity that decreased vital capacity. They were treated with nasal oxygen masks and active spirometry exercise without any further complications. There were 20 patients (10.4%) with persistent back pain and tingling or numbness in legs that affected their daily life infrequently. However, on further evaluating their MRI or CT scans there was no causative factors found out. They have been treated with medications, physiotherapy and reassurance. All patients were mobilized during the hospital stay with the help of physiotherapists after 24-48 hours of surgery as postoperative back pain was controlled. All patients were give training by physiotherapists for postural changes, mobilization, back strengthening exercises, toilet training and avoidance to bending forward and sitting on floor.
Discussion
Advances in pre-operative optimization, operative techniques and perioperative management have made surgical intervention a reasonable alternative for an increasing number of patients. Multiple investigators have reported substantial benefit of surgery with respect to pain, self-image, function, and ability to perform physical activities [10,15]. These benefits have been demonstrated despite the complexity of spinal realignment procedures and a substantial perioperative complication rate. There is a large body of evidence demonstrating positive mid- to long-term outcomes following surgical intervention for adult spinal deformity [16]. Yadla et al [10] found that operative intervention for adult spinal deformity is associated with improvement in both radiographic and clinical outcomes at a minimum 2-year follow-up. Similarly we have also found in our study that there was significant improvement in clinical as well as radiological parameters in our patient groups which has proven the benefits of surgery. In our study we have found overall 24.8% complications which is almost similar to the rate published in literature [1,12,13,17,18]. Postoperative deterioration in pulmonary functions in form of decrease in FEV1 is a major concern causing increased respiratory efforts and decreased oxygen saturation. There is an inevitable natural decline in pulmonary function with ageing, which may be more pronounced in patients with untreated spinal deformity [19]. Lehman et al. [20] demonstrated significant decline in all measures of pulmonary function (5-6% decline compared with predicted age-related decline) following deformity surgery with a clinically significant decline (a decline of >10% inFEV1) in pulmonary function in 27% of the patients of their series of 164 patients operated for adult spinal deformity. However, they did not evaluate immediate postoperative FEV1. In our series we have found decreased oxygen saturation and increased respiratory efforts postoperatively mainly due to obesity and post-operative pain as well as use of opioid analgesics which might cause respiratory depression. We therefore, give 30 degree prope-up position with nasal oxygen and encouragement of spirometry exercise once patient is able to follow the commands soon after surgery. With maintaining this protocol none of our patients had any long-term respiratory infections or difficulty. Additionally to start with preoperative spirometry exercise is also welcome to avoid and treat such conditions postoperatively. Proximal junctional kyphosis (PJK) or degeneration with implant loosening is also a known and well described complication in literature. In recent review article by Lau et al [17] suggested that the reported incidence of PJK ranged widely, from 5% to 46% in patients undergoing spinal instrumentation and fusion for adult spinal deformity. It is reported that 66% of PJK occurs within 3 months and 80% within 18 months after surgery. The reported revision rates due to PJK range from 13% to 55%. In our case series we have found over all 3.1% of proximal level problems and out of which we did revision surgery for five patients. One patient did not want to go ahead with revision surgery eventually developed spastic paraplegia. While other five patients who underwent revision surgery eventually improved without any further sequel. Additionally we have started Teriperatide injections to all of them to develop bone mass as their BMD suggested of having osteroporosis. Later on we have followed a protocol of starting Teriperatide injection (explained before surgery) postoperatively and maintaining that we had not found significant complications related with PJK [21,22]. Additionally we also explained our patients to avoid sitting of floor and bending forward to prevent PJK. In another review article by Soroceanu et al [23] included 245 patients to identify implant related complications after adult spinal deformity surgery. They found out 31.7% patients have had some sort of implant related complications and52.6% of those patients required reoperation. Rod breakage accounted for 47% of the implant-related complications, and proximal junctional kyphosis accounted for 54.5% of radiographical complications. In our series although we found out PJK, we did not find any patients have had complications such as rod breakage or mal-positioning of implants that needs revision. In another recent article by Sandquist et al. [24] suggested that their unique technique of multilevel segmental screw technique (MLSS) where a longer length pedicle screws was inserted from pedicle to upward direction crossing at least one or two segments to achieve stronger hold in one or two more vertebral levels; and thus decreasing chances of PJK in their series. However, we have not used this technique in any of our patients. There were other un-expected complications were also noted in our patient series such as acute renal shut down in one patient requiring hemodialysis. That patient was having hypertension as well as diabetes with renal compromise. Probable cause for ARF was identified as prolonged hypotension postoperatively has caused decreased renal perfusion resulting in to renal shut down. Therefore, we usually follow having blood pressure of minimum 100mm of Hg during surgery with constant watch on urine output. Postoperatively as well keeping Foley catheter in situ until patient starts walking and mobilizing to toilet would keep eye on volume and color of urine. If we feel color of urine is darker than what is expected, it would be always better to investigate for blood urea and creatinine level along with input output chart to correct immediately. There was one patient with acute pulmonary embolism postoperatively. Patient had long travel 24 hours before surgery with history of diabetes and previous heart disease. We then thereafter follow a protocol not to operate patients who have had long travel before 48 hours. We also investigate in form of venous Doppler study and postoperatively we also use DVT stockings to prevent such incidences unless patient starts walking independently postoperatively. We agree that this is a retrospective review study in patients with adult spinal deformity with primarily aimed at treating primary factors such as stenosis or instability along with correction of deformity. Minimum follow-up being only 12 months is also less if we wants to study all possible complications after such major surgery. However, large numbers of patient in our series is sufficient to explain and possible precautions to manage such patients postoperatively. Additionally our preoperative and postoperative precautionary steps in form of spirometry exercise, mobilization and anti DVT protocols, implementation of anti osteoporosis medications and avoidance as well as modification of life style might have prevented certain complications described in the literature. In spite of all shortcomings in the study, we think this would guide further to researchers and surgeons to keep complication rates lower after adult spinal deformity surgery.
References
1. Smith JS KM, Crawford A, Shaffrey CI. Outcomes, expectations and complication overview for the surgical treatment of adult and paediatric spinal deformity. Spine deformity preview 2012:4-14.
2. Federal interagency forum on aging-related statistics. Older American update: Key indicator of wellness. (<http://www.agingstats.gov/agingstatsdotnet/Main_site/Data/Data_2006.aspx>) 2006; [Accessed August 8, 2011 ].
3. Bess S, Boachie-Adjei O, Burton D, Cunningham M, Shaffrey C, Shelokov A, Hostin R, Schwab F, Wood K, Akbarnia B. Pain and disability determine treatment modality for older patients with adult scoliosis, while deformity guides treatment for younger patients. Spine (Phila Pa 1976) 2009;34:2186-90.
4. Glassman SD, Berven S, Kostuik J, Dimar JR, Horton WC, Bridwell K. Nonsurgical resource utilization in adult spinal deformity. Spine (Phila Pa 1976) 2006;31:941-7.
5. Simmons ED, Jr., Kowalski JM, Simmons EH. The results of surgical treatment for adult scoliosis. Spine (Phila Pa 1976) 1993;18:718-24.
6. Deyo RA, Ciol MA, Cherkin DC, Loeser JD, Bigos SJ. Lumbar spinal fusion. A cohort study of complications, reoperations, and resource use in the Medicare population. Spine (Phila Pa 1976) 1993;18:1463-70.
7. Bradford DS, Tay BK, Hu SS. Adult scoliosis: surgical indications, operative management, complications, and outcomes. Spine (Phila Pa 1976) 1999;24:2617-29.
8. Baron EM, Albert TJ. Medical complications of surgical treatment of adult spinal deformity and how to avoid them. Spine (Phila Pa 1976) 2006;31:S106-18.
9. Burneikiene S, Nelson EL, Mason A, Rajpal S, Serxner B, Villavicencio AT. Complications in patients undergoing combined transforaminal lumbar interbody fusion and posterior instrumentation with deformity correction for degenerative scoliosis and spinal stenosis. Surg Neurol Int;3:25.
10. Yadla S, Maltenfort MG, Ratliff JK, Harrop JS. Adult scoliosis surgery outcomes: a systematic review. Neurosurg Focus;28:E3.
11. Charosky S, Guigui P, Blamoutier A, Roussouly P, Chopin D. Complications and risk factors of primary adult scoliosis surgery: a multicenter study of 306 patients. Spine (Phila Pa 1976);37:693-700.
12. Daubs MD, Lenke LG, Cheh G, Stobbs G, Bridwell KH. Adult spinal deformity surgery: complications and outcomes in patients over age 60. Spine (Phila Pa 1976) 2007;32:2238-44.
13. Lonergan T, Place H, Taylor P. Acute Complications Following Adult Spinal Deformity Surgery in Patients Aged 70 Years and Older. J Spinal Disord Tech.
14. Modi HN, Suh SW, Hong JY, Cho JW, Park JH, Yang JH. Treatment and complications in flaccid neuromuscular scoliosis (Duchenne muscular dystrophy and spinal muscular atrophy) with posterior-only pedicle screw instrumentation. Eur Spine J;19:384-93.
15. Smith JS, Shaffrey CI, Glassman SD, Berven SH, Schwab FJ, Hamill CL, Horton WC, Ondra SL, Sansur CA, Bridwell KH. Risk-benefit assessment of surgery for adult scoliosis: an analysis based on patient age. Spine (Phila Pa 1976);36:817-24.
16. Paulus MC, Kalantar SB, Radcliff K. Cost and value of spinal deformity surgery. Spine (Phila Pa 1976);39:388-93.
17. Lau D, Clark AJ, Scheer JK, Daubs MD, Coe JD, Paonessa KJ, LaGrone MO, Kasten MD, Amaral RA, Trobisch PD, Lee JH, Fabris-Monterumici D, Anand N, Cree AK, Hart RA, Hey LA, Ames CP. Proximal junctional kyphosis and failure after spinal deformity surgery: a systematic review of the literature as a background to classification development. Spine (Phila Pa 1976);39:2093-102.
18. Shapiro GS, Taira G, Boachie-Adjei O. Results of surgical treatment of adult idiopathic scoliosis with low back pain and spinal stenosis: a study of long-term clinical radiographic outcomes. Spine (Phila Pa 1976) 2003;28:358-63.
19. Weinstein SL, Zavala DC, Ponseti IV. Idiopathic scoliosis: long-term follow-up and prognosis in untreated patients. J Bone Joint Surg Am 1981;63:702-12.
20. Lehman RA, Jr., Kang DG, Lenke LG, Stallbaumer JJ, Sides BA. Pulmonary function following adult spinal deformity surgery: minimum two-year follow-up. J Bone Joint Surg Am;97:32-9.
21. Ohtori S, Inoue G, Orita S, Yamauchi K, Eguchi Y, Ochiai N, Kishida S, Kuniyoshi K, Aoki Y, Nakamura J, Ishikawa T, Miyagi M, Kamoda H, Suzuki M, Kubota G, Sakuma Y, Oikawa Y, Inage K, Sainoh T, Takaso M, Toyone T, Takahashi K. Comparison of teriparatide and bisphosphonate treatment to reduce pedicle screw loosening after lumbar spinal fusion surgery in postmenopausal women with osteoporosis from a bone quality perspective. Spine (Phila Pa 1976);38:E487-92.
22. Park JH, Kang KC, Shin DE, Koh YG, Son JS, Kim BH. Preventive effects of conservative treatment with short-term teriparatide on the progression of vertebral body collapse after osteoporotic vertebral compression fracture. Osteoporos Int;25:613-8.
23. Soroceanu A, Diebo BG, Burton D, Smith JS, Deviren V, Shaffrey C, Kim HJ, Mundis G, Ames C, Errico T, Bess S, Hostin R, Hart R, Schwab F, Lafage V. Radiographical and Implant-Related Complications in Adult Spinal Deformity Surgery: Incidence, Patient Risk Factors, and Impact on Health-Related Quality of Life. Spine (Phila Pa 1976);40:1414-21.
24. Sandquist L, Carr D, Tong D, Gonda R, Soo TM. Preventing proximal junctional failure in long segmental instrumented cases of adult degenerative scoliosis using a multilevel stabilization screw technique. Surg Neurol Int;6:112.
| How to Cite this Article: Modi H, Dave BR. Complications encountered in surgical management adult spinal deformities- Prevention and management- a retrospective study in 193 patients. International Journal of Spine Apr – June 2016;1(1):21-24 . |

(Abstract) (Full Text HTML) (Download PDF)
Osteoporosis And its Effect on Progression of Adult Spinal Deformities
Volume 1 | Issue 1 |Apr – June 2016 | Page 15-20|H S Chhabra[1], PK Kartik Yelamarthy[1].
Authors :H S Chhabra[1], PK Kartik Yelamarthy[1]
[1] Indian Spinal Injuries Centre, Sector C, Vasant Kunj,
New Delhi, India.
Address of Correspondence
Dr. H S Chhabra
Indian Spinal Injuries Centre, Sector C, Vasant Kunj, New Delhi, India.
Email Id:-dryelamarthykarthik@gmail.com
Abstract
Adult spinal deformity may occur as the result of a number of conditions and patients may present with a heterogeneous group of symptoms. These include deformities in all 3 planes (coronal, sagital and axial) i.e scoliosis, kyphosis and rotational deformities. Clinical presentation varies and differs from pediatric deformities in that patients present more often with axial back pain and neurogenic claudication rather than a cosmetic deformity. Indications for treatment include pain, neurogenic symptoms, and progressive deformity. Larger deviations in the anterior, posterior or lateral plane will require greater energy use to maintain a standing position. Finally, progression outside of the “stable cone of economy” results in a loss of postural control and the need for external supports. The aim of this article is to analyze the role of osteoporosis in the progression of adult spinal deformity .We conducted a review of literature from Medline and searched for articles related to adult spinal deformities and osteoporosis. Osteoporosis along with progressive and asymmetric degeneration of the disc and facet joints has a role in progression of these deformities. Osteoporosis may also impact surgical options and can significantly impact the operative plan.
Keywords: Adult spinal deformity, osteoporosis, disc degeneration, deformity progression.
Introduction
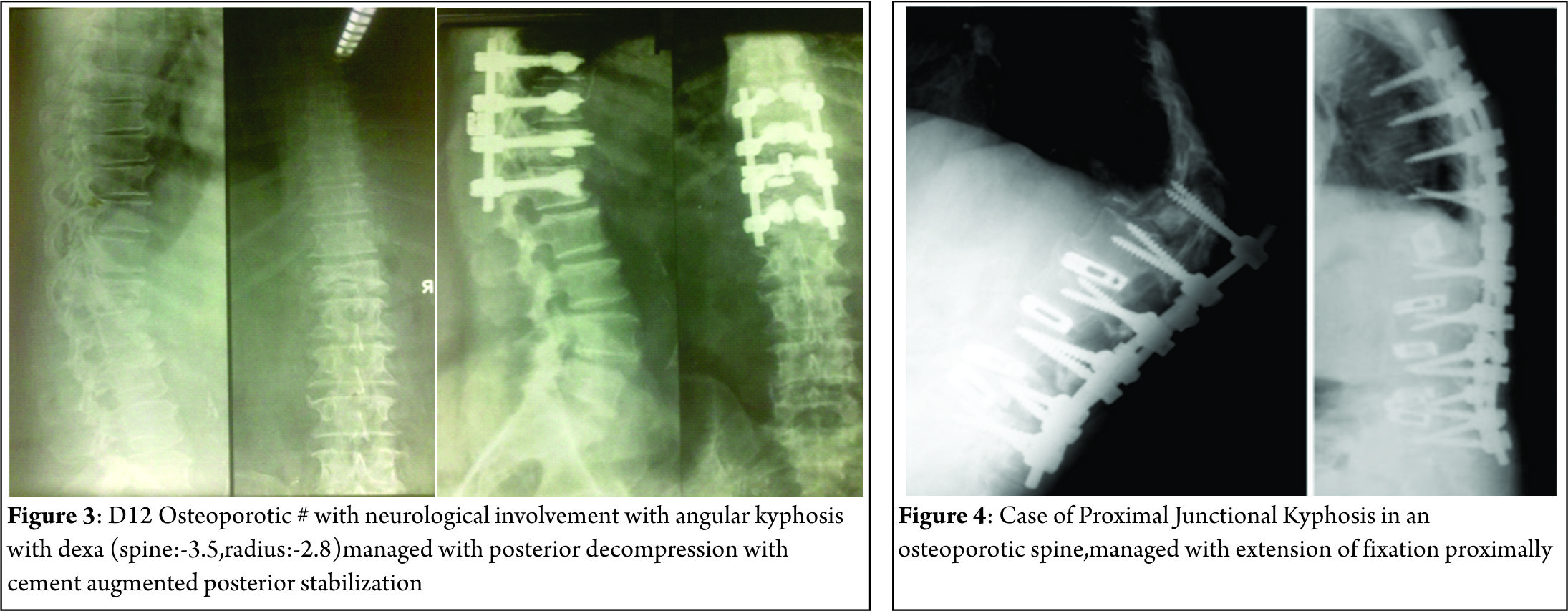
Spinal deformity is defined as a curvature in the spine where the alignment is outside of defined normal limits. Adult spinal deformity is one of the most challenging spinal disorders and by definition describes a complex spectrum of spinal deformities that present in adulthood including adult scoliosis, sagittal and coronal imbalance, and iatrogenic deformity, with or without spinal stenosis [1].Adult spinal deformity may occur as a result of a number of conditions, each of which ultimately lead to an imbalance of the structural support of the spinal column. Abnormal curvature may occur in the sagittal plane (kyphosis, lordosis) or in the coronal plane (scoliosis) causing imbalance in both planes . The magnitude of the curvature of the spine is measured using Cobb angle measurements. Axial plane deformity is measured by degrees of rotation from the frontal or sagittal plane [2]. Clinical presentation of adult spinal deformity varies greatly from minimal or no symptoms to severe pain with disability [3]. A majority of patients remain asymptomatic with radiographic findings alone. However, when patients begin to complain of symptoms, these may vary from mild back pain without radiculopathy to severe back pain with neurogenic claudication, radiculopathy, and walking intolerance.4 A complete patient assessment requires not only appropriate imaging studies but a complete history and physical exam. An adult deformity classification has been established by Schwab et al and applies radiographic parameters of disability[5]. As presented in Table 1. The presented adult deformity classification has a significant impact on surgical rates and operative strategy (approach, fusion to sacrum, and use of osteotomies). Through continued investigation, further refinement of the classification and formation of effective treatment algorithms are certain to emerge to guide the care of adults suffering from spinal deformity [5].
Scoliosis: A scoliosis is diagnosed in adult patients when it occurs or becomes relevant after skeletal maturity with a Cobb angle of more than 10 degrees in the frontal plain film [6,7].
Type 1: Primary degenerative scoliosis (‘‘de novo’’ form), mostly located in the thoracolumbar or lumbar spine
Type 2: Progressive idiopathic scoliosis in adult life of the thoracic, thoracolumbar, and/or lumbar spine
Type 3: Secondary degenerative scoliosis.
(a) Scoliosis following idiopathic or other forms of scoliosis or occurring in the context of a pelvic obliquity due to a leg length discrepancy, hip pathology or a lumbosacral transitional anomaly, mostly located in the thoracolumbar, lumbar or lumbosacral spine .
(b) Scoliosis secondary to metabolic bone disease (mostly osteoporosis) combined with asymmetric arthritic disease and/or vertebral fractures
Clinically, the most prominent groups are secondary (type 3) and primary (type 1)degenerative adult scoliosis. In elderly patients, all the three forms may be aggravated by osteoporosis [8,9,10].
Sagittal Plane Deformity: Age-related postural hyperkyphosis is an exaggerated anterior curvature of the thoracic spine, sometimes referred to as Dowager’s hump or gibbous deformity. This condition impairs mobility [22] and increases the risk of falls [23] and fractures [24]. Several types of postural deformities exist according to the number, severity, and location of vertebral fractures(upper or middle thoracic, thoracolumbar, or lumbar).Satoh et al. classified osteoporotic postural deformities into the following five groups based on changes of the physiological thoracic and lumbar curvature:[11]
1) normal posture without apparent change in spinal curve;
2) round back with increased thoracic kyphosis and normal lumbar lordosis;
3) hollow round back with increased thoracic kyphosis and lumbar lordosis;
4) whole kyphosis with extensive kyphosis from thoracic to lumbar spine; and
5) lower acute kyphosis with localized lumbar kyphosis with straight thoracic spine
Iatrogenic Spinal Deformity
Iatrogenic spinal deformities can cause either sagittal or coronal imbalance. They consist of flat back syndrome, post-laminectomy kyphosis and proximal junctional kyphosis(PJK).With the development of posterior segmental stabilization, the rates of flat back syndrome decreased [12,13,14,15,16]. A pathology known as junctional kyphosis also commonly calls for the use of instrumentation above the level of fusion in the thoraco-lumbar or cervico-thoracal vertebrae . Fusions that end at the level of the 7th and 8th thoracic vertebrae are known as the apex of thoracic kyphosis and may lead to junctional kyphosis. Post-laminectomy kyphosis is mostly seen after multi-level laminectomy procedures, especially in the cervical region and in cases of facetectomies with facet capsule destruction [17]. After cervical laminectomies in pediatric patients with incomplete bone development, post-laminectomy kyphosis is seen more commonly than in adult patients [17,18]. The rate of post-laminectomy kyphosis may become much greater in the population of pediatric patients with malignant intramedullary pathologies following radiotherapy treatment [17,19].
Natural History
Adult Scoliosis:
Idiopathic curves:(type 2 curves)[20]:
Lumbar curves of more than 300 degrees with apical vertebral rotation of more than 30% progressed the most. Right sided lumbar curves tended to progress twice as much as left lumbar curves. Also, marked vertebral rotation combined with translational shift (lateral olisthesis) was associated with significant curve progression. The thoracolumbar curve pattern manifested the most pronounced amount of apical vertebral rotation. The incidence of translatory shifts increased with time. Combined curves tended to balance with age, although lumbar part tended to progress more than the thoracic counter part. Weinstein and Ponsetti noted greater progression in lumbar curve if L5 was not well seated over the sacrum and apical vertebral rotation was more than 33% [48].
De novo curves (type 1 curves)[20]:
Robin et al analysed 554 individuals longitudinally for 7 to 13 years (315 women and 239 men, age range 50 to 84 yrs). 179 had curves exceeding 100. Fifty five (10%) developed denovo scoliosis during this period. Left sided curves were common in women. Sex ratio (F:M) increased with curve size. Rotatory olisthesis was found in 34% of patients, most common at L3-4 and L4-5 levels. As per a prospective study by Korovessis et al [21], risk factors directly related to curve progression were lateral olisthesis at the apical vertebra, a high Harrington factor (Cobb angle divided by number of vertebrae included in the curve) and the disc index.
Sagittal Plane Deformity:
The natural history of hyperkyphosis is not firmly established. Hyperkyphosis may develop from either muscle weakness and degenerative disc disease, leading to vertebral fractures and worsening hyperkyphosis, or from initial vertebral fractures that precipitate its development
Cause And Progression Of Adult Deformity (scoliosis, sagittal deformity, iatrogenic deformity)
Scoliosis:
The clinical syndrome of spinal osteoporosis is characterized by the occurrence of non-traumaticvertebral fractures and a disproportionately large amount of loss of trabecular bone necessary for the maintenance of vertebral strength [25,26].
Significant correlations exist between the bone mineral content, the compressive strength of the vertebrae [27,27,29], vertebral fractures, hyperkyphosis, and back pain. What remains unresolved is the role played by decreased vertebral bone mineral content in the development and progression of scoliosis in the adult. Shands and Eisberg noted a higher incidence of scoliosis in persons over 60years of age. Later, Vanderpool et al [30] reported scoliosis in 6%of persons over 50 years, and 36%more in those with osteoporosis. Those authors noted that scoliosis can arise in the elderly and is etiologically related to the higher incidence of metabolic bone disease. In an epidemiological study of routine anteropostenor (AP) chest and recumbent roentgenograms of the lower thoracic and lumbar spine, Robin et a1 .concluded that there was no basis for assuming a causal relationship between scoliosis and osteoporosis .But several theories could explain the association between fractures and scoliosis. Fractures may cause scoliosis, or, conversely scoliosis may cause fractures. Alternatively, scoliosis and fractures may be manifestations of the same underlying condition so that they would be expected to occur together frequently. The posterior spinal elements, facet joints. and ligamentous structures are not disrupted in osteoporotic compression fractures and may provide a fixed axis for sagittal and coronal spinal deformities. Yet this explanation does not account for the rotatory component of the deformity seen in osteoporotic patients. Mechanical factors that increase the forces applied to a vertebra increase the likelihood of that vertebra mechanically failing. Theoretically, a collagen abnormality may be responsible for osteoporosis and so called idiopathic scoliosis. Thus, several independent lines of evidence support the finding of a high concordance between osteoporosis and scoliosis. Fractures in osteoporotic or scoliotic patients would result from routine loading of an inherently weak spinal connective tissue [31].
The asymmetric degeneration of the disc and/or the facet joints leads to an asymmetric loading of the spinal segment and consequently of a whole spinal area. This again leads to an asymmetric deformity. Such a deformity again triggers asymmetric degeneration and induces asymmetric loading, creating a vicious cycle and enhancing curve progression. The destruction of structural spinal elements like discs, facet joints, and joint capsules responsible for stability leads to uni- or multi-segmental, multi-directional instability and can manifest as spondylolisthesis or translational or rotary olisthesis. The biological reaction is the formation of osteophytes at facet joint and vertebral end plates contributing to increasing narrowing of the spinal canal with facetjoint and ligamentum flavum hypertrophy and calcification. Effective narrowing of the spinal canal caliber causes central and lateral recess spinal stenosis [32,33]. Instability and collapse of the disc height leads to foraminal stenosis, with radicular pain or neurogenic claudication-type pain.
The asymmetric loading, coupled with degeneration, triggers a vicious cycle enhancing curve progression. This is fueled by common metabolic bone disorders like osteoporosis especially in post-menopause female patients leading to further asymmetric deformation and collapse in the weakened osteoporotic vertebra with subsequent curve progression[34].
Sagittal Plane Deformity:
Sagittal postural deformities begin with localized kyphosis due to either fracture or asymptomatic insidious collapse at the thoracic and/or thoracolumbar spine . This increased kyphosis (round back) can be readily compensated by increasing lumbar lordosis, resulting in the formation of the hollow round back [35]. Compensated upper thoracic lordosis for wedged vertebral fractures at the thoracolumbar junction results in lower acute kyphosis .If progressing round back cannot be compensated by lumbar lordosis, kyphosis extends down to the lumbar region, resulting in whole kyphosis. Therefore, whole kyphosis cannot be compensated by other spinal segments. Because lumbar kyphosis is thought to be related to weakness of the spinal extensors [36], whole kyphosis usually forces the patient to use a cane while standing and walking [35]. These uncompensated conditions seemed to contribute impairment of all the domain scores in the whole kyphosis group, especially in the activities of daily living domain score, resulting in a significant reduction in the total quality of life score compared with other postural deformities.
Iatrogenic Deformity:
Risk factors for PJK included age at operation, low bone mineral density, shorter fusion constructs, upper instrumented vertebrae below L2, and inadequate restoration of global sagittal balance. Osteopenia/osteoporosis has been established as a significant risk factor for proximal junctional kyphosis. Both symptomatic and asymptomatic compression fractures that kyphose the spine are not uncommon in the elderly. In addition, the elderly tend to have more kyphosis in their thoracic spine. For this reason, longer instrumented fusions that span the entire thoracic spine are often needed [37]
Implications of Deformity Progession:
In the domain of spinal surgery, it is useful to recall important concepts that can serve as a foundation to understanding and treating deformity. Optimal alignment of bone structures and joints is critical for the efficient function of the musculoskeletal system. Furthermore, a complex interaction of the neurologic system and muscular recruitment is necessary for ergonomic balance and deliberate displacement of the human body. Therefore, it is important to consider that ideal spinal alignment allows an individual to assume standing posture with minimal muscular energy expenditure. Physiologic curvatures of the spine in the sagittal plane, the straight spine in the coronal plane, balanced tension of the spinal ligaments, and activation of intrinsic anterior and posterior musculature should permit extended pain free erect position. This concept is reflected in the “Cone of Economy” principle conceptualized by Jean Dubousset [46] (Figure 1). Within the center of the cone, the individual may remain in an ergonomically favorable erect position. However, larger deviations in the anterior posterior
or lateral plane will require greater energy use to maintain a standing position. Finally, progression outside of the “stable cone” results in a loss of postural control and the need for external supports.

In the setting of adult spinal deformity (ASD), structural or iatrogenic modifications to spinal alignment should be considered . Spinal malalignment in ASD challenges balance mechanisms used for maintenance of an upright posture to achieve the basic human needs of preserving level visual gaze and retaining the head over the pelvis. Progressive severity in skeletal malalignment might result in greater recruitment in muscular effort and greater energy expenditure to maintain the erect posture as well as use of compensatory mechanisms. Spinal malalignment to the extremes of the “Cone of Economy” leads to extreme muscular demand, fatigue, and significant pain as well as disability. Once a spinal deformity has reached
the level of marked loss in function and quality of life, surgical intervention is often recommended and requested [46,47]
Influence of Osteoporosis on Management of Adult Deformity
The surgical treatment is complicated by the weak bone where implants are more difficult to be anchored and fixed, making the instrumented fusion prone to instrumentation-related complications. Trabecular bone is predominantly affected by osteoporosis, and because the pedicle screw has cortical contact limited to the pedicle isthmus, a “windshield wiper” mode of failure typically leads to screw loosening [38]. Therefore, fixation strategies for osteoporotic bone are targeted either toward taking advantage of the relatively stronger cortical bone [39] or toward augmenting the fixation of a pedicle screw within the existing trabecular bone [40]. It should be recognized, however, that when sclerosis is associated with degeneration in patients with adult scoliosis, the local bone mineral density may be significantly increased, limiting the local effects of the systemic osteoporosis. Various methods have been used for treatment of the osteoporotic patient, including sublaminar wires and pediculolaminar fixation [41], both of which take advantage of cortical bone composition of the posterior spinal lamina. In addition, techniques to improve the fixation of pedicle screws within osteoporotic trabecular bone have also been developed including polymethylmethacrylate cement augmentation of pedicle screws [42]. Calcium sulfate paste may also be used, which has the theoretical advantage of becoming replaced by bone over time 43. Other alternatives have been investigated, including conical screws, hydroxyapatite-coated screws, and expandable screws. There is no consensus on the optimal screw diameter, length, or shape for fixation in osteoporotic bone. It has been demonstrated that with high insertional torque, the screw-strength is improved [44]. This may be attained by undertapping (or not tapping) the screw trajectory. Larger-diameter screws may offer increased contact with the cortical bone of the pedicle and, thus, increase insertional torque. However, this may potentially increase the risk of pedicle fracture particularly in this population. Longer screw length also can increase screw pull-out strength, particularly when there is “bicortical” purchase with the distal end of the screw passing through the anterior vertebral cortex. However, bicortical purchase increases the possibility of injury to abdominal or vascular structures and therefore is usually limited to the sacral region. An additional strategy is to use multiple points of fixation with a numerous pedicle screw construct thus providing for the spread and distribution of contact forces. Care should be taken to preserve the supraspinous ligament, intraspinous ligament, and ligamentum flavum between the rostral fused level and the adjacent segment as well as throughout the construct where possible. This may possibly prevent the development of junctional deformity and instability because it serves as a segment of high posterior tension. With extension of the fusion to the sacrum, utilization of multiple and bicortical screw fixation in addition to consideration of anterior column support at L5–S1 and/or iliac fixation should be considered. Larger diameters and increased lengths to 70 or 80 mm improve iliac screw pull-out strength. This improved caudal fixation in deformity patients has been found to be persistent in patients with a minimum of 5 years of follow-up [45]. In summary, several of the central tenets of spinal reconstruction are particularly important in the adult deformity patient population with poor bone quality. Appropriate balance reduces junctional forces, which diminishes the risk of both instrumentation failure and adjacent vertebral fractures. The surgeon should thus endeavor to balance the rostral and caudal ends of the construct. In addition, a meticulous fusion procedure, augmented with appropriate bone graft or bone graft substitutes, is especially important. This will support the development of a rapid and solid fusion such that long-term spinal stability will be ensured, relieving the requirements put upon the reconstruction instrumentation and its relatively poor interface with the osteoporotic bone.
Conclusions
Adult spinal deformity may occur as a result of a number of
conditions, each of which ultimately lead to an imbalance of the
structural support of the spinal column. These deformities can
occur in all 3 planes. The asymmetric loading, coupled with
degeneration is fuelled by osteoporosis in the progression of
adult spinal deformities. Osteoporosis also plays a role in
deciding the instrumentation to be used in management of these deformities.
References
1. Birknes JK, White AP, Albert TJ, Shaffrey CI, Harrop JS. Adult degenerative scoliosis: a review. Neurosurgery 2008;63(3, Suppl): 94–103
2. Curr Rev Musculoskelet Med. 2011 Dec; 4(4): 159–167
3. Schwab F, Lafage V, Farcy JP, et al. Surgical rates and operative outcome analysis in thoracolumbar and lumbar major adult scoliosis: application of the new adult deformity classification. Spine 2007;32:2723–2730
4. Sengupta K. Adult spinal deformity. In: Rao RD, Smuck M, eds. Orthopaedic Knowledge Update: Spine, 4th ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2012:349–367
5. Schwab F, Lafage V, Farcy JP, Bridwell K, Glassman S, Ondra S, Lowe T, Shainline M. Surgical rates and operative outcome analysis in thoracolumbar and lumbar major adult scoliosis: application of the new adult deformity classification. Spine (Phila Pa 1976). 2007 Nov 15;32(24):2723-30.
6. Schwab F, el-Fegoun AB, Gamez L, Goodman H, Farcy JP. A lumbar classification of scoliosis in the adult patient: preliminary approach. Spine (Phila Pa 1976). 2005 Jul 15;30(14):1670-3.
7. Aebi M. The adult scoliosis. Eur Spine J. 2005 Dec;14(10):925-48
8. Grubb SA, Lipscomb HJ. Diagnostic findings in painful adult scoliosis. Spine (Phila Pa 1976). 1992 May;17(5):518-27.
9. Healey JH, Lane JM. Structural scoliosis in osteoporotic women. Clin Orthop Relat Res. 1985 May;(195):216-23
10. Velis KP, Healey JH, Schneider R. Osteoporosis in unstable adult scoliosis. Clin Orthop Relat Res. 1988 Dec;(237):132-41.
11. Satoh K, Kasama F, Itoi E, et al. Clinical features of spinal osteoporosis: spinal deformity and pertinent back pain. Contemp Orthop. 1988;16:23–30
12. Bridwell KH, Betz R, Capelli AM, Huss G, Harvey C. Sagittal plane analysis in idiopathic scoliosis patients treated with Cotrel-Dubousset instrumentation. Spine (Phila Pa 1976). 1990 Sep;15(9):921-6.
13. Lenke LG, Bridwell KH, Baldus C, Blanke K, Schoenecker PL. Ability of Cotrel-Dubousset instrumentation to preserve distal lumbar motion segments in adolescent idiopathic scoliosis. J Spinal Disord. 1993 Aug;6(4):339-50.
14. Lenke LG, Bridwell KH, Baldus C, Blanke K, Schoenecker PL. Cotrel-Dubousset instrumentation for adolescent idiopathic scoliosis. J Bone Joint Surg Am. 1992 Aug;74(7):1056-67
15. Takahashi S, Delécrin J, Passuti N. Changes in the unfused lumbar spine in patients with idiopathic scoliosis. A 5- to 9-year assessment after cotrel-dubousset instrumentation. Spine (Phila Pa 1976). 1997 Mar 1;22(5):517-23
16. Wiggins WC, Ondra SL, Shaffray CI. Management of flat-back syndrome. Neurological Focus 2003; 15(3): 1-9.
17. Deutsch H, Haid RW, Rodts GE, Mummaneni PV. Postlaminectomy cervical deformity. Neurosurg Focus 2003;15(3): E5
18. Katsumi Y, Honma T, Nakamura T: Analysis of cervical instability resulting from laminectomies for removal of spinal cord tumor. Spine 1989;14:1171–1176.
19. Yeh JS, Sgouros S, Walsh AR, Hockley AD. Spinal sagittal malalignment following surgery for primary intramedullary tumours in children. Pediatr Neurosurg. 2001 Dec;35(6):318-24
20. The Lumbar Spine edited by Harry N. Herkowitz, International Society for Study of the Lumbar Spine
21. Korovessis P, Piperos G, Sidiropoulos P, Dimas A. Adult idiopathic lumbar scoliosis. A formula for prediction of progression and review of the literature. Spine (Phila Pa 1976). 1994 Sep 1;19(17):1926-32.
22. Kado DM, Huang MH, Barrett-Connor E, Greendale GA. Hyperkyphotic posture and poor
physical functional ability in older community-dwelling men and women: the Rancho Bernardo
study. J Gerontol A Biol Sci Med Sci 2005;60:633–637.
23. Kado DM, Huang MH, Nguyen CB, Barrett-Connor E, Greendale GA. Hyperkyphotic posture and risk of injurious falls in older persons: the Rancho Bernardo Study. J Gerontol A Biol Sci Med Sci 2007;62:652–657
24. Huang MH, Barrett-Connor E, Greendale GA, Kado DM. Hyperkyphotic posture and risk of future osteoporotic fractures: the Rancho Bernardo study. J Bone Miner Res 2006;21:419–423
25. Mazess RB. Measurement of skeletal status by noninvasive methods. Calcif Tissue Int. 1979 Oct 31;28(2):89-92.
26. Nordin BE. Clinical significance and pathogenesis of osteoporosis. Br Med J. 1971 Mar 13;1(5749):571-6.
27. Hansson T, Roos B. Microcalluses of the trabeculae in lumbar vertebrae and their relation to the bone mineral content. Spine (Phila Pa 1976). 1981 Jul-Aug;6(4):375-80..
28. Hansson T, Roos B, Nachemson A. The bone mineral content and ultimate compressive strength of lumbar vertebrae. Spine (Phila Pa 1976). 1980 Jan-Feb;5(1):46-55..
29. Hansson T, Roos B. The relation between bone mineral content, experimental compression fractures, and disc degeneration in lumbar vertebrae. Spine (Phila Pa 1976). 1981 Mar-Apr;6(2):147-53.
30. Vanderpool DW, James JI, Wynne-Davies R. Scoliosis in the elderly. J Bone Joint Surg Am. 1969 Apr;51(3):446-55
31. Healey JH, Lane JM. Structural scoliosis in osteoporotic women. Clin Orthop Relat Res. 1985 May;(195):216-23
32.Benner B, Ehni G. Degenerative lumbar scoliosis. Spine 1979; 4:548
33. Ploumis A, Transfledt EE, Denis F. Degenerative lumbar scoliosis associated with spinal stenosis. Spine J. 2007 Jul-Aug;7(4):428-36.
34. Kotwal S, Pumberger M, Hughes A, Girardi F. Degenerative scoliosis: a review. HSS J. 2011 Oct;7(3):257-64.
35. Satoh K, Kasama F, Itoi E et al. Clinical features of spinal osteoporosis: spinal deformity and pertinent back pain. Contemp Orthop 1988;(16):23–30
36. Takemitsu Y, Harada Y, Iwahara T, Miyamoto M, Miyatake Y. Lumbar degenerative kyphosis. Clinical, radiological and epidemiological studies. Spine (Phila Pa 1976). 1988 Nov;13(11):1317-26.
37. Lau D, Clark AJ, Scheer JK, Daubs MD, Coe JD, Paonessa KJ, LaGrone MO, Kasten MD, Amaral RA, Trobisch PD, Lee JH, Fabris-Monterumici D, Anand N, Cree AK, Hart RA, Hey LA, Ames CP; SRS Adult Spinal Deformity Committee. Proximal junctional kyphosis and failure after spinal deformity surgery: a systematic review of the literature as a background to classification development. Spine (Phila Pa 1976). 2014 Dec 1;39(25):2093-102.
38. Law M, Tencer AF, Anderson PA. Caudo-cephalad loading of pedicle screws: mechanisms of loosening and methods of augmentation. Spine (Phila Pa 1976). 1993 Dec;18(16):2438-43.
39. Coe JD, Warden KE, Herzig MA, McAfee PC. Influence of bone mineral density on the fixation of thoracolumbar implants. A comparative study of transpedicular screws, laminar hooks, and spinous process wires. Spine (Phila Pa 1976). 1990 Sep;15(9):902-7.
40. Tan JS, Kwon BK, Dvorak MF, Fisher CG, Oxland TR. Pedicle screw motion in the osteoporotic spine after augmentation with laminar hooks, sublaminar wires, or calcium phosphate cement: a comparative analysis. Spine (Phila Pa 1976). 2004 Aug 15;29(16):1723-30.
41. Hilibrand AS, Moore DC, Graziano GP. The role of pediculolaminar fixation in compromised pedicle bone. Spine (Phila Pa 1976). 1996 Feb 15;21(4):445-51..
42. Sarzier JS, Evans AJ, Cahill DW. Increased pedicle screw pullout strength with vertebroplasty augmentation in osteoporotic spines. J Neurosurg. 2002 Apr;96(3 Suppl):309-12
43. Rohmiller MT, Schwalm D, Glattes RC, Elalayli TG, Spengler DM. Evaluation of calcium sulfate paste for augmentation of lumbar pedicle screw pullout strength. Spine J. 2002 Jul-Aug;2(4):255-60..
44. Zindrick MR, Wiltse LL, Widell EH, Thomas JC, Holland WR, Field BT, Spencer CW. A biomechanical study of intrapeduncular screw fixation in the lumbosacral spine. Clin Orthop Relat Res. 1986 Feb;(203):99-112..
45. Tsuchiya K, Bridwell KH, Kuklo TR, Lenke LG, Baldus C. Minimum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine (Phila Pa 1976). 2006 Feb 1;31(3):303-8.
46. Dubousset J. Three-dimensional analysis of the scoliotic deformity. In: Weinstein SL, ed. Pediatric Spine: Principles and Practice. New York, NY: Raven Press; 1994
47. Schwab F, Patel A, Ungar B, Farcy JP, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2224-31.
48. Weinstein SL, Ponseti IV: Curve progression in idiopathic scoliosis. J Bone Joint Surg Am. 1983, 65: 447-455
| How to Cite this Article: Chhabra HS, Yelamarthy PKK. Osteoporosis and its effect on progression of Adult Spinal deformities. International Journal of Spine Apr – June 2016;1(1):15-20 . |

(Abstract) (Full Text HTML) (Download PDF)
Golden Era for Spine Advancements
Volume 1 | Issue 1 | Apr – June 2016 | Page 1-2|Ketan Khurjekar[1], Shailesh Hadgaonkar[1], Ashok Shyam[1,2]
Authors :Ketan Khurjekar[1], Shailesh Hadgaonkar[1], Ashok Shyam[1],[2]
[1] Sancheti Institute for Orthopaedics &Rehabilitation, Pune, India
[2] Indian Orthopaedic Research Group, Thane, India
Address of Correspondence
IJS Editorial Officie
A-203, Manthan Apts, Shreesh CHS, Hajuri Road, Thane [W]
Maharashtra, India.
Email: editor.ijspine@gmail.com
Spine surgery is at the cross roads and spine healthcare in India is growing steadily. Indian medical system is golden combination of all medical systems across the globe. Today India is the second most populous country in the world and leader in healthcare provider. Spine surgery practices in tier 1 and tier 2 cities in India are at par with the world standard and surgeons from these cities are making spine surgery feasible and affordable in smaller towns and cities as well. Most of the Spine Surgeons have undergone vigorous spine surgery training in India and in Western countries. They have mastered the skill sets and are now delivering it back home in India. The volume of cases every health care professional is tackling is sharpening their skills and making them master on global platform. Structured training which every Spine Surgeon has gone through and seen across the globe has been accepted and also imparted in India. Organisations like Association of Spine Surgeons of India, National Board of Examinations and AO Spine India have started long term spine surgery training programme to impart knowledge to young aspiring surgeons. Strong leadership from these organisation has helped develop comradeship among spine surgeons and sharing of knowledge. Gaining knowledge and imparting it to eligible candidate, creates more knowledge. That is exactly happening in India. Most spine surgeons are following good practices, and are applying their expertise for betterment of the society. It is not enough just to have skills and man power, we need good operation rooms, and we need best of anaesthetist and intensivist to enhance the result of challenging spine surgery cases. More important, to sustain good results of any surgery, we need good quality armamentaria, high definition microscopic Systems, advanced instrumentation systems and well equipped operation rooms. Today we have most of these things available at centres where spine patients are routinely operated. Even the smaller Hospital units are well equipped with most of the above necessary things. For the instance, a scoliosis surgery done in New York or a Cervical pedicle screw surgery done in Japan is been carried out exactly in the same manner with the same precision, with similar armamentaria and with the same implants in India. This scenario is giving confidence to the society; it is helping people to accept Spine surgery. We believe this is one of the most important change where spine surgery is rapidly gaining acceptance amongst all strate of society. Spine surgery was considered as taboo for many years and today situation is changing fast. With expert surgeons, good infrastructure the spine surgeries have become safer and has invoked confidence from our patients. We are standing at the Golden Era of Spine Advancement in the Country. Why our setups are unique, special and also appreciated internationally? Because we are delivering World class health care at affordable price. We have seen steady growth of spine surgery but we need to do more to achieve excellence. We have to reach out to masses with same precision and equal efficacy. Task is daunting but not impossible. We neither have National Health system, nor do we have majority population having individual Insurance protection. In India around 10 % population has personal Insurance coverage. But every person has access to affordable world class medical system. Affluent class and higher middle class person from the society gets a spine surgery done from a corporate set up, lower middle class personal has easy access to nursing home and weaker section of the society goes to Government, municipal or public hospital. The health care professional working in a municipal hospital is of a meritorious background. The surgical skills imparted are of high standards. No one is deprived of his own right. In NHS, one may have to wait for more than six months to get the surgery done while in some other country the Surgery may not be possible without sufficient insurance protection. We are doing the service to society without diluting precision in the surgery. Excellence in medical practices can be achieved by expertise in that particular field, structured training of that specialty, advanced technology based armamentaria and research. We have achieved first three things satisfactorily but research is yet to be in motion. To do so, we need to inculcate the habit of maintaining our registry, we need to establish data keeping system and preserve the record of every surgery to learn from these experiences. The next generation will stand tall on the shoulder of its predecessors. We are on the right path, but a lot of distance is yet to be covered. Starting this, International Spine Journal aims at establishing strong roots of research. ‘Training and Research by Publishing’ is the main goal of the Journal. It will be an exercise to inculcate the habit of maintaining records. Training through research will be a motto for next decade. Documentation and Research, the fourth dimension of achieving medical excellence is paramount to achieve Safe Spine Surgery.
Dr. Ketan Khurjekar | Dr. Shailesh Hadgaonkar | Dr. Ashok Shyam
| How to Cite this Article: Khurjekar K, Hadgaonkar S, Shyam A. Golden Era for Spine Advancements. International Journal of Spine Apr – June 2016;1(1):1-2 . |

(Abstract) (Full Text HTML) (Download PDF)
Decision Making in Surgical Management of Degenerative Scoliosis
Volume 1 | Issue 1 | Apr – June 2016 | Page 10-14|Kunal Shah[1], Manish Kothari[1], Abhay Nene[1].
Authors :Kunal Shah[1], Manish Kothari[1], Abhay Nene[1]
[1] Department of Spine Surgery, Wockhardt Hospital and Medical Research Centre Agripada, Dr Anand Rao Nair Road
Mumbai Central, Mumbai. India – 400008.
Address of Correspondence
Dr. Abhay Nene
Department of Spine Surgery, Wockhardt Hospital and Medical Research Centre Agripada, Dr Anand Rao Nair Road,Mumbai Central, Mumbai. India – 400008
Email: abhaynene@yahoo.com
Abstract
Surgical management of degenerative scoliosis has no established guidelines. The options available range from decompression alone, decompression with limited fusion or decompression with global fusion. Major factors influencing the type of surgery are symptomatology, spinal deformity, and general condition of patient and local factors in spine. Selection of surgical option and also outcome of surgical options depend on radiological and clinical factors. Radiological factors affecting surgery are magnitude of curve, apical vertebra rotation or subluxation and sagittal imbalance. Clinical factors affecting outcome of surgery are amount of back pain compared to leg pain, patient willing to take risk of fusion surgery later, patient understanding of residual back pain, complications of surgery and general condition to cope with the surgery. Therefore a balance between benefits of surgery and complications should be evaluated before choosing the type of surgery. In this article we share our experience with literature review in management of such complex situations.
Keywords: Adult degenrative scoliosis, decision making, management.
Introduction
The type of surgery to be performed in degenerative scoliosis is always been controversial. There is no general consensus on one type of surgery better than other. The goal of surgery is to relieve the leg pain/back pain and correct sagittal/coronal imbalance. The surgery can range from decompression alone, decompression with limited fusion or decompression with global fusion. The decision of type of surgery should be taken with all considerations based on clinical profile of patients, amount of restriction daily activities, general condition of patient and expectation out of surgery, so as to choose the most suitable surgery under given circumstances. Major factors influencing the type of surgery are symptomatology, spinal deformity, and general condition of patient and local factors in spine.
1) Symptomatology
Clinical presentation is variable ranging from no symptoms or minimal symptoms to severe pain associated with disability. Mainly the symptoms are deformity, back pain and radiculopathy/claudication or weakness. Back pain is the most common symptom of presentation in degenerative scoliosis. Pain is directly related to amount of degeneration of intervertebral disc and facet joints. Pain is not directly related to the size of curve, but associated with sagittal imbalance [1, 2]. Leg pain and neurological claudication are primary symptoms of degenerative scoliosis. Foraminal stenosis is most common in concave side of the curve caused due to facetal hypertrophy and lateral translation of vertebral body. Convex side symptoms are rare and can be attributed to stretching of nerve. Sagittal imbalance causes muscle fatigue and subsequent back pain [3, 4]. Surgery is usually indicated in cases with severe radiculopathy or neurodeficit, affecting daily activities. Therefore all kind of surgery requires decompression to free the nerve either foraminal or central. Decompression alone has a fear of curve progression, worsening of vertebral body subluxation and persistent back pain [4]. Therefore addition of fusion surgery is advocated. However either local or global fusion is associated with morbidity especially in elderly patients [5]
2) Patient profile
Degenerative scoliosis is usually seen in elderly .Therefore general condition of patient in view of medical complications and co morbidities should be evaluated [4]. In frail elderly, operative time, amount of blood loss and extent of surgery should be considered to prevent perioperative morbidity. Minimal short time surgery is preferred in elderly frail patients.
3) Spinal deformity
In degenerative scoliosis, the curves are stiffer and require extensive surgery for correction as compared to adolescent scoliosis. Surgery for coronal plane deformity is indicated in unbalanced curves, progression of curve and large curves and rarely for cosmetic reasons [6]. However associated sagittal plane deformity can also cause symptoms of back pain and leg pain. Inability to restore sagittal balance leads to poor surgical outcome. Sagittal decompensation due to inadequate correction can be associated with higher pelvic incidence and pelvic tilt. Therefore lumbar lordosis should be corrected in proportion to the pelvic incidence. Inadequate correction of lumbar lordosis is also seen with loss of correction of disc spaces after posterior instrumentation. Anterior column reconstruction prevents loss of correction of disc spaces and gives better restoration of lumbar lordosis [7]. Therefore the type of surgery should also aim at restoring sagittal balance.
4) Local factors
Osteoporosis is one of the major concerns in treatment of degenerative scoliosis. It is usually associated with loss of fixation and pseudoarthrosis. Use of cement with screws or additional anterior column support to augment posterior fixation helps in preventing complications [4].We believe that taking above factors in consideration and aim of restoration of coronal and sagittal imbalance with minimal surgical intervention is the key to successful outcome in degenerative scoliosis. The real answered question arises is that should the surgery be decompression alone or it should be combined with fusion (local or global) and levels of fusion
Decompression alone
Decompression alone is indicated when primary complaints is radiculopathy/claudication with minimal or no back pain. Radiographically these are typically smaller curves without any instability. This approach gives dramatic pain relief in leg symptoms and improves walking distance [8]. The concerns with decompression alone are possibility of further progression of deformity or iatrogenic spinal instability [9]. It serves as a good option in elderly patients who cannot tolerate fusion surgery. Liu et al [10] in a study of 112 patients operated for degenerative scoliosis concluded that the patients operated with decompression alone gives satisfactory results and type of surgery should be based on patient’s age, general and economic factors, severity of deformity and other coexisting lumbar degenerative disorders. Hosogane et al [11] concluded that average curve progression was 3.4 degree in mean follow up of 2.8 years in patients operated with decompression alone. In only 21.6 % patients the curve progressed to more than 5 degrees. This progression was similar to curve progression in natural history of degenerative scoliosis. Curve progression after decompression surgery alone could not be predicted in preoperative period. They concluded that fusion surgery is not always advocated to prevent curve progression when the main symptoms of patients are due to nerve compression. Matsumura et al [12] studied results of microscopic bilateral decompression via a unilateral approach (MBDU) in degenerative lumbar scoliosis. They concluded that MBDU reduces postoperative segmental instability and achieve satisfactory clinical outcome, convex approach gives good visibility of neural structures and facet joint. Figure 1 shows a 67 year old lady with multiple co morbidities and osteoporosis, complaining of severe neurogenic claudication with no back pain. Radiograph showed degenerative scoliosis and a stable spondylolisthesis at L45 level. MRI was suggestive of significant L45 level compression. Her daily functional demands were less .She was operated with decompression at L4-5 level.
. MRI showed significant c ompression at l4-5 level (c). She was operated with decompression alone surgery")
Decompression with limited fusion
Decompression with limited fusion is usually indicated in cases having single level instability or to prevent iatrogenic instability in the decompressed area. It is a good option in moderate curve with segmental instability. The concerns with limited fusion are adjacent segment disease which is commonly seen. If the fusion stops at the apex of deformity, then deformity might increase [5].
Figure 2 shows a case of 60 year old lady with significant back pain and localized nerve symptoms; radiograph showed a degenerative scoliosis with Cobb angle of 35 degrees and L4-5 instability with significant localized compression on MRI. She was operated with decompression with L4-5 fusion.
Decompression with global fusion
Decompression with global fusion is indicated when there is large curve and apical vertebra subluxation. The symptoms are disabling with significant back pain with leg pain. Posterior instrumentation gives good coronal correction but poor sagittal correction. Adequate restoration of sagittal balance requires anterior column support or vertebral osteotomy procedures [5, 13, 14].
Anterior alone surgery has advantages of enhanced fusion rates due to large surface area, better global curve correction and preservation of posterior musculature. However it is associated with high complication rates and morbidity especially in elderly. Combined anterior and posterior surgery is associated with better curve correction, higher fusion rates and better restoration of sagittal and coronal imbalance. However it is associated with increase in operative time, more blood loss and morbidity [15, 16,17].
Crandall and Revella [18] compared results of anterior interbody fusion versus posterior interbody fusion in treatment of degenerative scoliosis. They found no significant difference in clinical outcomes or complication rates.
Surgical correction of sagittal deformity is described using various osteotomy procedures like Smith –Peterson osteotomy, pedicle subtraction osteotomy and vertebral column resection. When deciding on the osteotomies, advantages should be weighed against the morbidity [8].
Cho et al [5] in a comparative study between short fusion versus long fusion in degenerative scoliosis concluded that long fusion gave better correction of scoliotic curve, coronal imbalance and rotational subluxation of apical vertebra as compared to short fusion. However sagittal balance and lumbar lordosis was inadequately corrected.
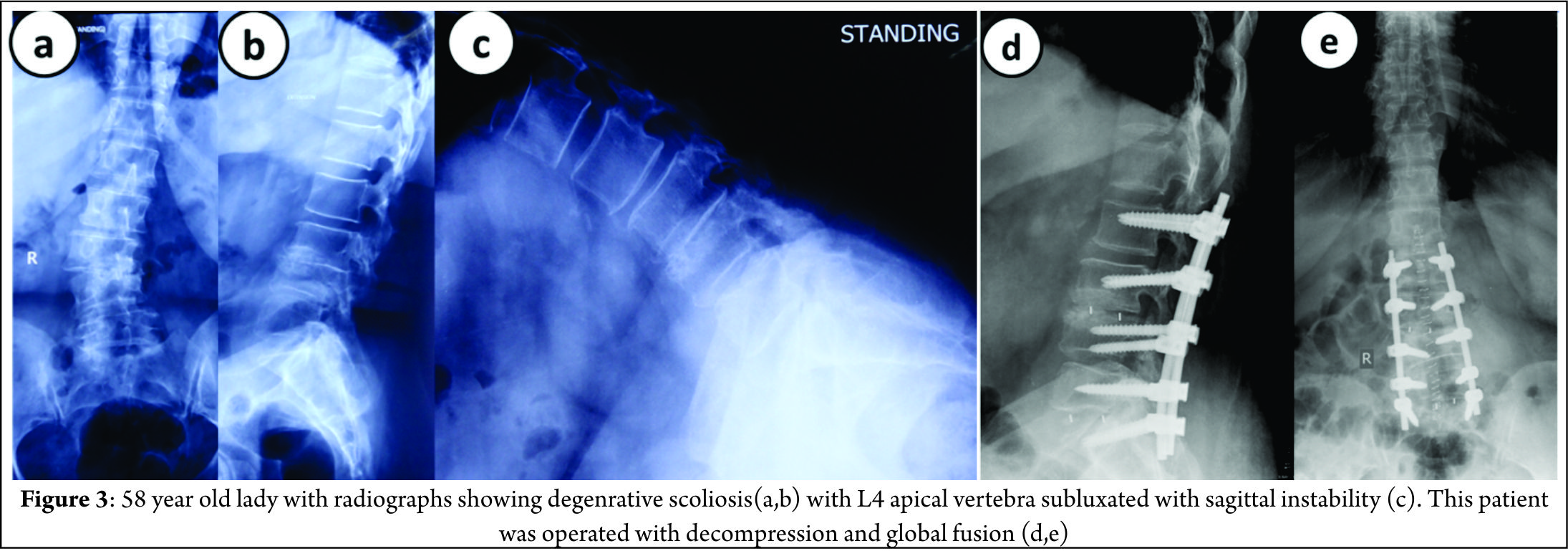
Figure 3 shows a 58 year old lady with significant back pain and leg pain, radiographs shows degenerative scoliosis with Cobb angle of 45 degrees, L4 vertebra (apical vertebra) subluxated with sagittal instability. She was operated with decompression at L45 with posterior global correction.
Levels of fusion
General guidelines for fusion should be followed to prevent complications [19,20].
1) These are the fusion should not stop at apex or at spondylolisthesis.
2) Junction kyphosis should be included
3) Retrolisthesis or anterolisthesis should be included and
4) Laterally translated vertebra or level of rotatoy subluxation should be included in fixation.
5) Usually the upper instrumented vertebra should be the most horizontal vertebra.
Proximal extent
The proximal extent of fusion is debatable and there is controversy whether the fusion should stop at lumbar level, T11/T12 or T10.
Fusion stopping at L1 can cause adjacent segment disease due to high stresses in proximal junction area. Therefore it is recommended to fuse above. Some authors suggest that it does not prevent adjacent segment disease (ASD) because ASD is a part of degenerative process [21]. Extension of fusion upto T10 as against stopping at T11/T12 is favored since T10 is more stable due to true rib attachment. Fusion upto T10 is associated with high perioperative complications due to extensive surgery. Some authors suggest that T11/T12 level is acceptable if the upper instrumented vertebra is above upper end vertebra [22].
Distal extent
Fusion upto sacrum is recommended when L5-S1 segment has some pre-existing pathology. Controversy arises when L5-S1 segment is healthy [23]. Advantages of fusion upto sacrum are better correction of sagittal imbalance and no chances of subsequent degeneration. Disadvantages of fusion upto sacrum are it’s a relatively morbid procedure and high chances of pseudoarthrosis which can require subsequent extension of fusion upto ilium. Advantages of fusion upto L5 are that it is relatively less morbid and normal L5-S1 segment is spared. Disadvantage is that L5-S1 segment is prone to degeneration (ASD) [24,25].
Complications
Early
Early complications include pulmonary embolism, respiratory distress, epidural hematoma, transient neurologic deficit and infection. Risk factors for perioperative complications increase with longer operative time, excess blood loss, associated medical comorbidities and medications taken prior to surgery (ecosprin or clopidogrel).This can be prevented by optimizing patient well and shorter duration surgery with less blood loss [26,27]. Cho et al concluded that longer fusion group is associated higher rate of early complications [5].
Late
1) Adjacent segment disease
ASD presents as adjacent level stenosis and proximal junctional kyphosis. ASD can be caused due to facet joint violation, inadequate restoration of sagittal balance, stopping at junctional level (L1 or L5) and not including adjacent spondylolisthesis or apex in fixation[28,29]. ASD is common in short fusion group. ASD can be prevented by restoring sagittal balance and including high stress segments into fixation.
2) Pseudoarthrosis
Pseudoarthrosis is usually occurs at T12-L1 and L5-S1 junction. Risk factors for pseudoarthrosis are inadequate restoration of lumbar lordosis, osteoporosis and thoracolumbar kyphosis more than 20 degrees [30]. It can be prevented by including junctional area in fixation, restoring lumbar lordosis, creating larger surface area for fusion by anterior column grafting and use of artificial bone grafts or allografts.
3) Instrumentation failure
Instrumentation failure usually presents as screw loosening and screw pullout either at proximal or distal end. Risk factors for instrumentation failure are inadequate fixation, osteoporosis and inadequate sagittal balance restoration especially in long fixations [31,32]. This can be prevented by extending fusion upto ilium or using cemented screws.
Conclusions
Management of degenerative scoliosis is one of the most challenging issues in spine care and requires complex decision making in terms of treatment options and outcomes. Type of surgery depends on various radiological factors and clinical factors. Radiological factors affecting surgery are magnitude of curve, apical vertebra rotation or subluxation and sagittal imbalance. Clinical factors affecting surgery are amount of back pain compared to leg pain, patient willing to take risk of fusion surgery later, patient understanding of residual back pain, complications of surgery and general condition to cope with the surgery. Therefore a balance between benefits of surgery and complications should be evaluated before choosing the type of surgery.
References
1. Glassman SD, Bridwell K, Dimar JR, Horton W, Berven S, Schwab F. The impact of positive sagittal balance in adult spinal deformity. Spine (Phila Pa 1976) 2005;30:2024-9.
2. Palmisani M, Dema E, Cervellati S. Surgical treatment of adult degenerative scoliosis. Eur Spine J. 2013 Nov;22 Suppl 6:S829-33.
3. Simmons ED. Surgical treatment of patients with lumbar spinal stenosis with associated scoliosis. Clin Orthop Relat Res 2001;(384):45-53.
4. Cho KJ, Kim YT, Shin SH, Suk SI. Surgical treatment of adult degenerative scoliosis. Asian Spine J. 2014 Jun;8(3):371-81.
5. Cho KJ, Suk SI, Park SR, Kim JH, Kim SS, Lee TJ, Lee JJ, Lee JM. Short fusion versus long fusion for degenerative lumbar scoliosis. Eur Spine J. 2008 May;17(5):650-6.
6. Palmisani M, Dema E, Cervellati S. Surgical treatment of adult degenerative scoliosis. European Spine Journal. 2013;22(Suppl 6):829-833.
7. Cho KJ, Kim KT, Kim WJ, et al. Pedicle subtraction osteotomy in elderly patients with degenerative sagittal imbalance. Spine (Phila Pa 1976) 2013;38:E1561-6.
8. Youssef JA, Orndorff DO, Patty CA, Scott MA, Price HL, Hamlin LF, Williams TL, Uribe JS, Deviren V. Current status of adult spinal deformity. Global Spine J. 2013 Mar;3(1):51-62.
9. Vaccaro AR, Ball ST. Indications for instrumentation in degenerative lumbar spinal disorders. Orthopedics 2000;23:260-71.
10. Liu W, Chen XS, Jia LS, Song DW. The clinical features and surgical treatment of degenerative lumbar scoliosis: a review of 112 patients. Orthop Surg. 2009 Aug;1(3):176-83.
11. Hosogane N, Watanabe K, Kono H, Saito M, Toyama Y, Matsumoto M. Curve progression after decompression surgery in patients with mild degenerative scoliosis. J Neurosurg Spine. 2013 Apr;18(4):321-6.
12. Matsumura A, Namikawa T, Terai H, Tsujio T, Suzuki A, Dozono S, Yasuda H, Nakamura H. The influence of approach side on facet preservation in microscopic bilateral decompression via a unilateral approach for degenerative lumbar scoliosis. Clinical article. J Neurosurg Spine. 2010 Dec;13(6):758-65.
13. Bradford DS, Tribus CB. Vertebral column resection for the treatment of rigid coronal decompensation. Spine (Phila Pa 1976) 1997;22:1590-9.
14. Daffner SD, Vaccaro AR. Adult degenerative lumbar scoliosis. Am J Orthop (Belle Mead NJ) 2003;32:77- 82.
15. Than KD,Wang AC, Rahman SU, et al. Complication avoidance and management in anterior lumbar interbody fusion. Neurosurg Focus 2011;31:E6
16. Mundis GM, Akbarnia BA, Phillips FM. Adult deformity correction through minimally invasive lateral approach techniques. Spine 2010;35(26, Suppl):S312–S321
17. Jarrett CD, Heller JG, Tsai L. Anterior exposure of the lumbar spine with and without an “access surgeon”: morbidity analysis of 265 consecutive cases. J Spinal Disord Tech 2009;22:559–564
18. Crandall DG, Revella J. Transforaminal lumbar interbody fusion versus anterior lumbar interbody fusion as an adjunct to posterior instrumented correction of degenerative lumbar scoliosis: three year clinical and radiographic outcomes. Spine 2009;34:2126–2133
19. Aebi M. The adult scoliosis. Eur Spine J 2005;14:925- 48.
20. Gupta MC. Degenerative scoliosis. Options for surgical management. Orthop Clin North Am 2003;34:269-79.
21. Shufflebarger H, Suk SI, Mardjetko S. Debate: determining the upper instrumented vertebra in the management of adult degenerative scoliosis: stopping at T10 versus L1. Spine (Phila Pa 1976) 2006;31(19 Suppl):S185-94.
22. Cho KJ, Suk SI, Park SR, Kim JH, Jung JH. Selection of proximal fusion level for adult degenerative lumbar scoliosis. Eur Spine J 2013;22:394-401.
23. Polly DW Jr, Hamill CL, Bridwell KH. Debate: to fuse or not to fuse to the sacrum, the fate of the L5-S1 disc. Spine (Phila Pa 1976) 2006;31(19 Suppl): S179-84.
24. Edwards CC 2nd, Bridwell KH, Patel A, et al. Thoracolumbar deformity arthrodesis to L5 in adults: the fate of the L5-S1 disc. Spine (Phila Pa 1976) 2003; 28:2122-31.
25. Cho KJ, Suk SI, Park SR, et al. Arthrodesis to L5 versus S1 in long instrumentation and fusion for degenerative lumbar scoliosis. Eur Spine J 2009;18:531-7.
26. Gupta MC. Degenerative scoliosis. Options for surgical management. Orthop Clin North Am 2003;34:269–279
27. Mok JM, Cloyd JM, Bradford DS, et al. Reoperation after primary fusion for adult spinal deformity: rate, reason, and timing. Spine 2009;34:832–839
28. Kim YJ, Bridwell KH, Lenke LG, Rhim S, Cheh G. Sagittal thoracic decompensation following long adult lumbar spinal instrumentation and fusion to L5 or S1: causes, prevalence, and risk factor analysis. Spine (Phila Pa 1976) 2006;31:2359-66.
29. Cho KJ, Suk SI, Park SR, et al. Risk factors of sagittal decompensation after long posterior instrumentation and fusion for degenerative lumbar scoliosis. Spine (Phila Pa 1976) 2010;35:1595-601.
30. Kim YJ, Bridwell KH, Lenke LG, Cho KJ, Edwards CC 2nd, Rinella AS. Pseudarthrosis in adult spinal deformity following multisegmental instrumentationand arthrodesis. J Bone Joint Surg Am 2006;88:721- 8.
31. Emami A, Deviren V, Berven S, Smith JA, Hu SS, Bradford DS. Outcome and complications of long fusions to the sacrum in adult spine deformity: luquegalveston, combined iliac and sacral screws, and sacral fixation. Spine (Phila Pa 1976) 2002;27:776-86.
32. Tsuchiya K, Bridwell KH, Kuklo TR, Lenke LG, Baldus C. Minimum 5-year analysis of L5-S1 fusion using sacropelvic fixation (bilateral S1 and iliac screws) for spinal deformity. Spine (Phila Pa 1976) 2006;31:303-8.
| How to Cite this Article:Shah K, Kothari M, Nene A. Decision Making in Surgical Management of Degenerative Scoliosis. International Journal of Spine Apr – June 2016;1(1):10-14 . |
(Abstract) (Full Text HTML) (Download PDF)
Factors Influencing Sagittal Malalignment and its Effect on Clinical Implications in Adult Spinal Deformity
Volume 1 | Issue 1 | Apr – June 2016 | Page 5-9|Bassel G Diebo[1], Jeffrey J Varghese BS[1], Frank J Schwab[1].
Authors :Bassel G Diebo[1], Jeffrey J Varghese BS[1], Frank J Schwab[1].
[1]Department Spine Service, Hospital for Special Surgery, New York, NY, United States
Address of Correspondence
Dr. Bassel G. Diebo
Spine Service, Hospital for Special Surgery, New York, NY, United States.
Email: dr.basseldiebo@gmail.com
Abstract
Respect for the sagittal plane has been broadly published and accessible for all surgeons. Yet, suboptimal outcomes and revision cases remain highly prevalent. In this article, the authors present a case of a pleasant lady who started with a simple lumbar decompression surgery for spinal stenosis that deteriorated and then failed revision surgery, ultimately presenting with a severely disabling flatback and a remarkable spinal deformity. Her case highlights the importance of sagittal alignment in degenerative patients. Failure to appreciate the sagittal plane has a direct impact on patient reported outcomes and serious debilitating iatrogenic deformity. The maintenance of spinal alignment is not a deformity specific exercise; therefore, all surgeons should consider optimizing the sagittal plane to reduce the incidence of not only iatrogenic deformity but the burden of any spinal pathology.
Keywords: Sagittal Malalignment, adult spinal deformity, degenerative scoliosis.
Introduction
The close relationship between sagittal spinal alignment and patient reported outcomes is widely recognized [1–8]. As a result, sagittal radiographic parameters, such as the SRS-Schwab modifiers (Sagittal vertical axis: SVA, pelvic incidence minus lumber lordosis: PI-LL, and pelvic tilt: PT), have been investigated and validated in multiple spinal pathologies and patient groups. However, to date, iatrogenic causes remain an important contributor to the prevalence of adult spinal deformity. One reason for the increased incidence of iatrogenic deformity relates to the lack of correction and/or preservation of sagittal alignment when addressing focal or regional degenerative conditions. In addition to decompression and stabilization, maintenance of lumbar lordosis is crucial in avoiding the creation of deformities such as flatback syndrome [9]. The importance of the sagittal plane was originally established based on multi-center databases of spinal deformity patients; however, recent studies on patients undergoing less invasive procedures for lumbar degenerative conditions unraveled the universality of this importance. In a literature review of the last two decades, Mehta et al concluded that the sagittal parameters play a central role in the treatment of isthmic spondylolysis, spondylolisthesis, and degenerative pathologies [10]. Masevnin and Kumar et al have both demonstrated that adjacent segment pathologies are more prevalent in patients who underwent surgical correction of degenerative conditions without correcting sagittal alignment [11,12]. Finally, hypo- and hyperlordosis have been reported as risk factors for disc height reduction and facet joints arthritis, respectively [13,14]. Respect for the sagittal plane has been broadly published and accessible for all surgeons. Yet, suboptimal outcomes and revision cases remain highly prevalent [15–19]. In this article, the authors present a case of a pleasant lady who started with a simple lumbar decompression surgery and a subsequent failed revision surgery. Following a short fusion of L3-L5, the patient presented herself to the spine clinic of the senior author with a disabling flatback, an inability to walk more than 1 block, and a remarkable adult spinal deformity.
Case presentation:
History of present illness and physical examination:
This is a 70-year old Caucasian female who recently presented to the senior author’s clinic with a long history of back pain and two previous surgeries. In 2011, she had lumbar laminectomies and decompressions (L3-L5) and in 2012 she ultimately underwent a L3 to L5 instrumented fusion. Her severe (8/10) pain returned in 2013, originating in her buttock region, and traveled inferiorly through the right leg to the foot. For two years, the patient was only able to walk one block before she had to pitch forward from significant back pain and need external support. She underwent several non-operative treatments including: epidural injections, physical therapy, acupuncture, massages, and multiple nerve blocks. She is on Tramadol three times a day and one Percocet 5/325 every night. The patient stood with both sagittal and coronal malalignments (Fig. 1), was unable to toe or heel walk, and had poor tandem gait. She demonstrated right distal extremity numbness and weaknesses of both the tibialis anterior and extensor hallucis longus, but was otherwise neurovascularly intact.
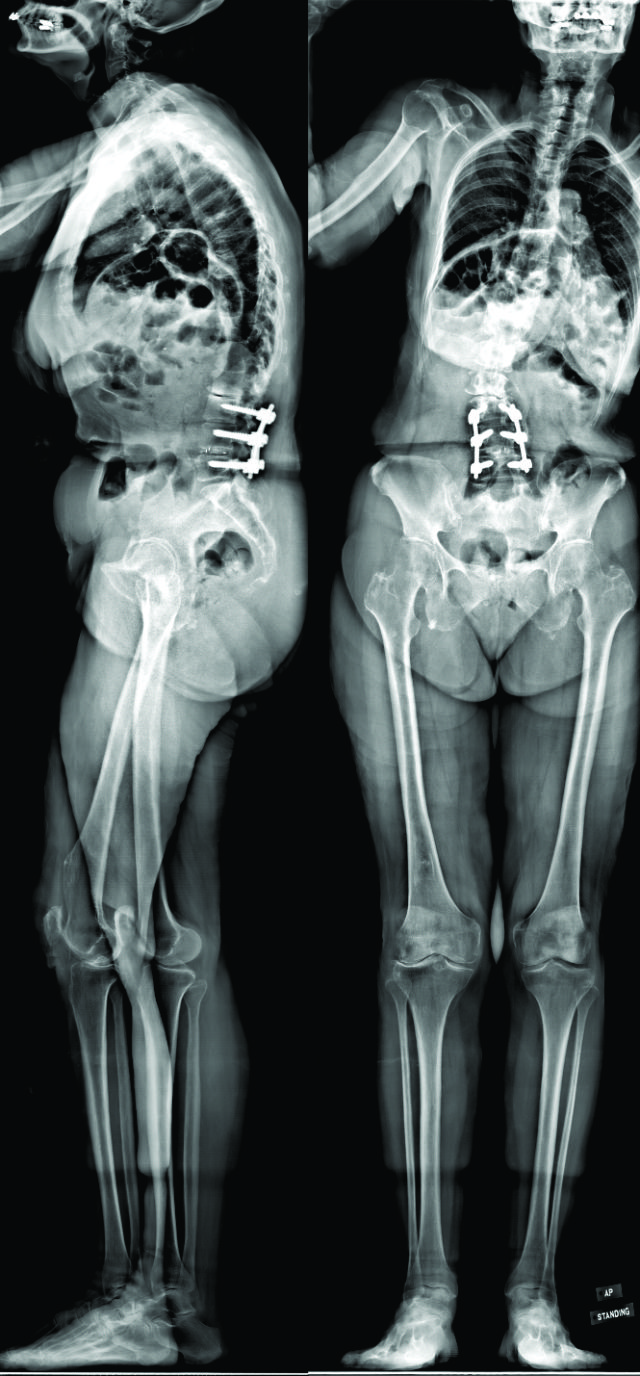
Figure 1: Pre-operative anterio-posterior and lateral radiographs
Radiographic imaging:
CT scan:T12-Sacrum axial imaging revealed a mild degenerative scoliosis of the upper lumbar spine with the apex between L2-L3. Cephalad to the L3-L5 fusion, the patient had facet arthroses, a disc bulge, and central canal stenoses at T12-L1 and L1-L2. At the fusion levels, the patient had multiple degenerative discs, facet arthroses, and neural foraminal narrowings. X-Ray analysis: The patient presented with a pelvic incidence of 57°, indicating a standard pelvic morphology from a spinal perspective. Sagittal alignment analysis revealed a severe adult spinal deformity classified by the SRS-Schwab: PI-LL mismatch of 34° (++), PT of 40° (++) and SVA of 86 mm (++). Thorough analysis of the lumbar spine demonstrated a caudal (L4-S1) lordosis of 24°, L3-L5 (fused segments) lordosis of 18° and, L1-L2 (unfused segments) kyphosis of 6° (Fig. 2). The thoracic spine did not exhibit any hypokyphotic compensation (TK = 45°). Coronal x-rays revealed a 22° coronal curve (L1-L3) and a 65 mm right coronal malalignment. The full radiographic analysis is reported in Fig. 3.
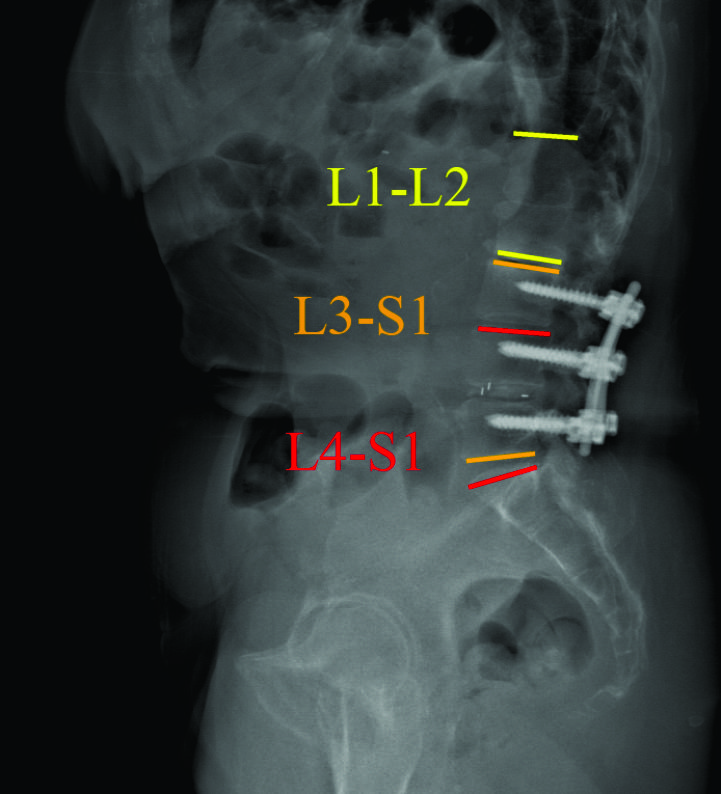
Figure 2: Pre-operative sagittal radiographic analysis

Figure 3: Pre-operative segmental analysis of lumbar lordosis
Surgical planning and technique:
After discussing the treatment options, benefits, and risks, with the patient for her severe sagittal plane deformity, the decision was made to extend the fusion to T3 with pelvic fixation. The surgical strategy included a L3 pedicle subtraction osteotomy (PSO) of 35° and a L5-S1 transpedicular lumbar interbody fusion (TLIF) for an expected 10° of lordotic correction. Using dedicated software (Surgimap, Nemaris Inc, New York, NY), the surgical plan was simulated to ensure proper post-operative alignment. Patient-specific custom rods were generated and forwarded to the manufacturer to be pre-bent, ensuring an accurate execution of the surgical plan. In the OR, the reconstruction required additional T3-L2 Smith-Peterson osteotomies to afford fusion and deformity correction. At the osteotomy site, a wide laminar foraminotomy from L2 to L4 was performed and two short rods were added between these levels (Four-Rod technique), offering adequate correction and closure. Fluoroscopy confirmed that the proper correction was achieved in both planes.
Post-operative follow-up:
The patient recovered without incident, and is not only satisfied but happy with her new posture. Radiographic analysis revealed an adequate lumbar lordosis, a PI-LL within 10 degrees, a global sagittal alignment (SVA) of 36 mm, and a pelvic tilt of 28°. These are classified as (0), (0) and (+) based on SRS-Schwab classification. The lumbar coronal curve was corrected to 8 degrees and the C7PL to 16 mm to the right. (Fig 4)
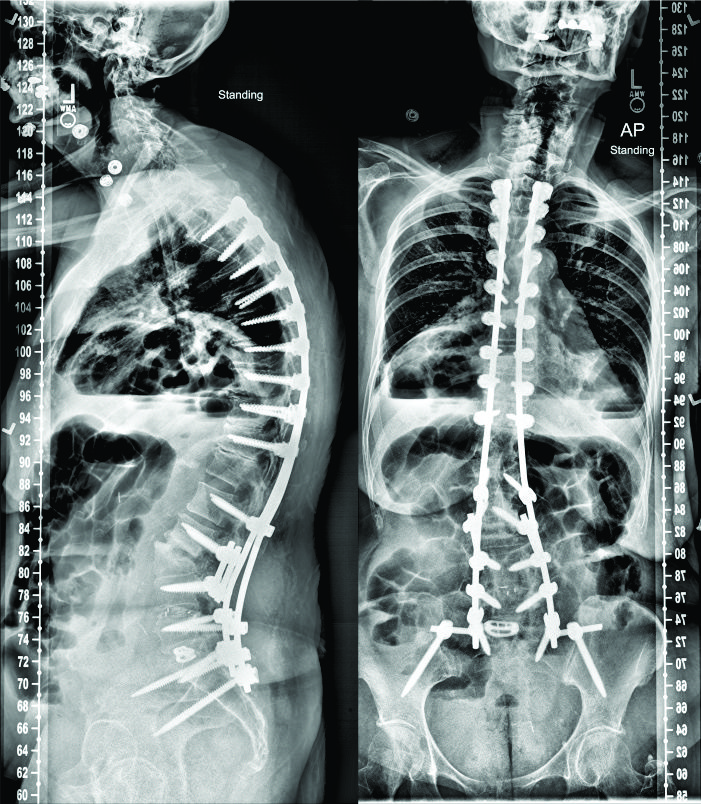
Figure 4: Post-operative anterio-posterior and lateral radiographs
Discussion:
There is a growing body of evidence in the literature regarding the clinical implications of sagittal spinal alignment. Over the last decade, scientific conferences are increasingly dedicating significant amounts of time and effort to raising awareness and spreading the sagittal message. The teaching today is: optimize or preserve the sagittal alignment of the spine in all spectrums of operations, from ‘simple’ one-level fusions to complex multi-planar deformity surgeries. For the management of spinal pathologies, it is no longer acceptable to perform only neural decompressions for stenosis and only fusions for stabilizing the spine. The sagittal plane, specifically with respect to lumbar lordosis, should be optimally aligned, if not already. This recommendation is valid almost regardless of the spinal etiology. To guide spinal realignment in adult spinal deformity, the key sagittal modifiers (PT, PI-LL, and SVA), with their clinically relevant thresholds, are already cornerstones for surgical correction. These parameters are also being investigated in patients with degenerative disc diseases, spondylolisthesis (degenerative and isthmic), as well as spinal stenosis. Moving beyond deformity: sagittal alignment in degenerative diseases:
In degenerative spondylolisthesis (DS), it is now established that higher pelvic incidences result in higher sacral slopes and shear stresses at the lumbosacral junction, making it a predisposing factor for DS. Moreover, Jeon et al took this a step further to conclude that degenerative retrolisthesis exists in two types, both of which are driven by sagittal parameters; one primarily resulting from degeneration in patients with low pelvic incidences, and the other secondarily resulting from compensatory mechanisms in patients with anterolistheses and high pelvic incidences [20]. Ultimately, sagittal alignment influences two out of the three features included in the Labelle classification of spondylolisthesis [21]. With regards to surgical treatment, Feng et al showed that the restoration of pelvic tilt and lumbar lordosis played important roles in the surgical outcomes of DS [22]. In other degenerative diseases, Bae et al demonstrated that patients with an upper lumbar disc herniation have significantly different sagittal profiles than patients with a lower disc herniation. In their studies, pelvic incidence and lumbar lordosis were significantly factors in determining the level of disc herniation [23)]. Thus, treatment of these pathologies is increasingly considering the sagittal plane.
Sagittal alignment in spinal stenosis:
Patients with lumbar stenosis adopt a forward compensatory bending posture to relieve the symptoms of neural compression [25,26].This malalignment pattern may be confused with sagittal spinal deformity and a loss of lumbar lordosis. Thus, there has been a recent debate on whether a surgeon should address the stenosis by decompression+/-fusion alone or with spinal realignment as well. Recent data demonstrated that decompression alone does indeed improve the sagittal profile of spinal stenosis patients. Jeon et al investigated 40 lumbar stenosis patients and followed them up to two years. In their study, patients who underwent decompressions alone had improvements in SVA, from 39 mm at baseline to 23 mm at 2 year follow up [24]. Buckland et al, in unpublished data, showed that while anterior truncal malalignment was similar between deformity and degenerative patients, pelvic tilt appeared to be a unique compensatory mechanism of deformity patients. Recently, Fujii et al showed that decompressions can improve global alignment in stenotic patients when malalignment is induced by a compensatory reduction in lumbar lordosis [27]. However, they also noticed that without corrective surgery, stenosis patients with higher preoperative malalignments (PI-LL > 21.5 and SVA > 69 mm) had residual malalignments postoperatively. This malalignment has proven to negatively impact patients reported outcomes in another study by Hikata et al [28)] In general, there is rising consensus that lumbar stenosis patients with severe sagittal malalignment (SRS Schwab SVA ++) should be assessed for a concomitant sagittal deformity and ultimately be considered for corrective surgery.
While more research is needed to establish treatment guidelines for sagittal realignment of spinal stenosis patients, it is crucial to understand that the maintenance of sagittal alignment is a must. The patient in this article deteriorated from being a spinal stenosis patient undergoing a two-level fusion to a flatback patient requiring realignment with osteotomy. This iatrogenic deformity is challenging and is commonly seen in daily practice of deformity surgeons. Based on the PI-LL formula, our patient needed approximately 50° of L1-S1 lordosis, of which 65% (32°) should be in the extreme caudal lumbar segments [29)]. However, when looking at the L1-S1 lordosis of this patient, she only had 21°. More importantly, the previously fused caudal segments were constructed with only 18°, which is a clear loss of lordosis.
Sagittal alignment: How to improve, What is new and How to be more patient-specific?
To improve our understanding of the sagittal plane, the gap between researchers and clinicians must be bridged. Feedback from surgeons in daily practice is crucial to improve the current guidelines of sagittal realignment. The ultimate goal is a personalized treatment that addresses the patient’s age, pathology, function, expectations, and spino-pelvic morphology.
Lafage et al investigated the impact of age on the spino-pelvic alignment and provided updated thresholds of PT, PI-LL and SVA [30]. The new targets for the radiographic parameters provide more “patient-specific” alignment thresholds. Their data revealed that age should be considered when determining the ideal sagittal alignment for a given patient, with older patients requiring less rigorous alignment objectives (Table 1).
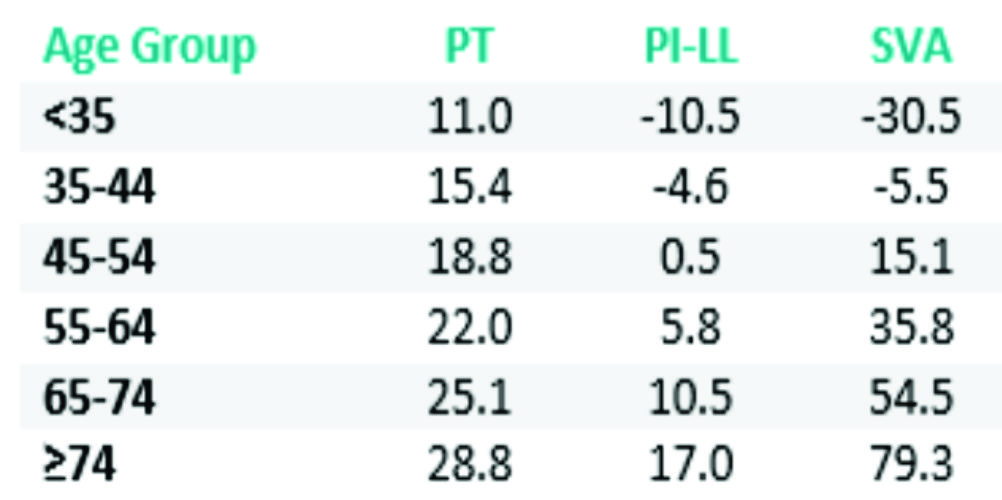
Table 1: Age-adjusted sagittal alignment thresholds.
Moreover, patient-specific instrumentation is a recent advancement in spine surgery. Surgeons can now plan their surgery and choose or construct certain instrumentations based on their patient’s morphology and alignment targets. Using the existing knowledge on the optimal sagittal alignment, these customized implants might help preserve the sagittal plane in degenerative patients. There are several factors that need to be acknowledged to achieve or maintain adequate sagittal alignment of the spine. The pelvis is a key component that must be considered. The measurement of pelvic incidence (PI) and the calculation of the mismatch between PI and lumbar lordosis are crucial in assessing the deformity magnitude when its main driver is the loss of LL. Any mismatch > 10° is associated with worse patient reported outcomes. Every surgeon needs to ensure that the surgical intervention does not alter this harmony between the spine and the pelvis [1,4]. Moreover, analysis of the compensatory mechanisms recruited by each patient is mandatory. Pelvic tilt, thoracic hypokyphosis, and knee flexion [31] are common mechanisms that need to be considered and delineated from the main driver of deformity. The surgery needs to be planned with the help of dedicated software and the plan needs to be simulated to confirm that post-operative alignment is ideal [32,33]. Finally, patient expectations, comorbidities, and their soft tissue profile are highly important aspects to consider. These are being investigated for their impact on how we treat our spinal pathology patients.
Conclusions
This article, drawing support from cases and the plethora of literature available, highlights the importance of sagittal alignment in degenerative patients. Failure to appreciate the sagittal plane has a direct impact on patient reported outcomes and serious debilitating iatrogenic deformity. The maintenance of spinal alignment is not a deformity specific exercise; therefore, all surgeons should consider optimizing the sagittal plane to reduce the incidence of not only iatrogenic deformity but the burden of any spinal pathology.
References
1. Schwab F, Patel A, Ungar B, Farcy J, Lafage V. Adult spinal deformity-postoperative standing imbalance: how much can you tolerate? An overview of key parameters in assessing alignment and planning corrective surgery. Spine (Phila Pa 1976). 2010 Dec;35(25):2224–31.
2. Schwab FJ, Lafage V, Farcy J-P, Bridwell KH, Glassman SD, Ondra S, et al. Surgical rates and operative outcome analysis in thoracolumbar and lumbar major adult scoliosis: application of the new adult deformity classification. Spine (Phila Pa 1976) [Internet]. 2007 Nov 15;32(24):2723–30.
3. Youssef J a, Orndorff DO, Patty C a, Scott M a, Price HL, Hamlin LF, et al. Current Status of Adult Spinal Deformity. Glob spine J [Internet]. 2013 Mar;3(1):51–62.
4. Schwab FJ, Ungar B, Blondel B, Buchowski J, Coe J, Deinlein D, et al. Scoliosis Research Society-Schwab adult spinal deformity classification: a validation study. Spine (Phila Pa 1976) [Internet]. 2012 May 20 [cited 2013 Aug 12];37(12):1077–82.
5. Terran J, Schwab F, Shaffrey CI, Smith JS, Devos P, Ames CP, et al. The SRS-schwab adult spinal deformity classification: Assessment and clinical correlations based on a prospective operative and nonoperative cohort. Neurosurgery. 2013 Jul;73(4):559–68.
6. Sengupta DK. Re: Schwab F, Ungar B, Blondel B, et al. Scoliosis research society—Schwab adult spinal deformity classification–-a validation study. Spine 2012; 37:1077—82. Spine (Phila Pa 1976) [Internet]. 2012 Sep 15 [cited 2014 Mar 24];37(20):1790.
7. Smith JS, Klineberg E, Schwab F, Shaffrey CI, Moal B, Ames CP, et al. Change in Classification Grade by the SRS-Schwab Adult Spinal Deformity Classification Predicts Impact on Health-Related Quality of Life Measures: Prospective Analysis of Operative and Non-operative Treatment. Spine (Phila Pa 1976). 2013;38:1663–71.
8. Hallager DW, Hansen LV, Dragsted CR, Peytz N, Gehrchen M, Dahl B. A comprehensive analysis of the SRS-Schwab Adult Spinal Deformity Classification and confounding variables – a prospective, non-US cross-sectional study in 292 patients. Spine (Phila Pa 1976) [Internet]. 2015 Dec 9;
9. Farcy J-P, Schwab FJ. Management of flatback and related kyphotic decompensation syndromes. Spine (Phila Pa 1976) [Internet]. 1997 Oct;22(20):2452–7.
10. Mehta V a., Amin A, Omeis I, Gokaslan ZL, Gottfried ON. Implications of spinopelvic alignment for the spine surgeon. Neurosurgery [Internet]. 2011 Mar [cited 2014 Nov 18];70(3):707–21.
11. Masevnin S, Ptashnikov D, Michaylov D, Meng H, Smekalenkov O, Zaborovskii N. Risk factors for adjacent segment disease development after lumbar fusion. Asian Spine J [Internet]. 2015 Apr;9(2):239–44.
12. Kumar M, Baklanov A, Chopin D. Correlation between sagittal plane changes and adjacent segment degeneration following lumbar spine fusion. Eur Spine J [Internet]. 2001 Aug 1 [cited 2014 Nov 18];10(4):314–9.
13. Inoue G, Takaso M, Miyagi M, Kamoda H, Ishikawa T, Nakazawa T, et al. Risk Factors for L5-S1 Disk Height Reduction after Lumbar Posterolateral Floating Fusion Surgery. J Spinal Disord Tech [Internet]. 2014;27(5):187–92.
14. Jentzsch T, Geiger J, König M a, Werner CML. Hyperlordosis Is Associated With Facet Joint Pathology At The Lower Lumbar Spine. J Spinal Disord Tech [Internet]. 2013;
16. Maier SP, Lafage V, Smith JS, Obeid I, Mundis GM, Klineberg EO, et al. Revision Surgery After Three-Column Osteotomy (3CO) in 335 Adult Spinal Deformity (ASD) Patients: Intercenter Variability and Risk Factors. Spine J [Internet]. 2013 Sep [cited 2013 Dec 5];13(9):S9–10.
17. Sansur C a, Reames DL, Smith JS, Hamilton DK, Berven SH, Broadstone P a, et al. Morbidity and mortality in the surgical treatment of 10,242 adults with spondylolisthesis. J Neurosurg Spine [Internet]. 2010 Nov [cited 2014 Jun 10];13(5):589–93.
18. Diebo BG, Henry J, Lafage V, Berjano P. Sagittal deformities of the spine: factors influencing the outcomes and complications. Eur Spine J [Internet]. 2015 Jan [cited 2015 Mar 10];24 Suppl 1:3–15.
19. Diebo BG, Passias PG, Marascalchi BJ, Jalai CM, Worley NJ, Errico TJ, et al. Primary Versus Revision Surgery in the Setting of Adult Spinal Deformity: A Nationwide Study on 10,912 Patients. Spine (Phila Pa 1976) [Internet]. 2015;
20. Jeon CH, Park JU, Chung NS, Son KH, Lee YS, Kim JJ. Degenerative retrolisthesis: Is it a compensatory mechanism for sagittal imbalance? Bone Jt J. 2013;95 B(9):1244–9.
21. Labelle H, Mac-Thiong J-M, Roussouly P. Spino-pelvic sagittal balance of spondylolisthesis: a review and classification. Eur Spine J [Internet]. 2011 Sep [cited 2013 Oct 7];20 Suppl 5:641–6.
22. Feng Y, Chen L, Gu Y, Zhang Z-M, Yang H-L, Tang T-S. Influence of the posterior lumbar interbody fusion on the sagittal spino-pelvic parameters in isthmic L5-s1 spondylolisthesis. J Spinal Disord Tech [Internet]. Elsevier Inc; 2014;27(1):E20–5.
23. Bae J, Lee S-H, Shin S-H, Seo JS, Kim KH, Jang J-S. Radiological analysis of upper lumbar disc herniation and spinopelvic sagittal alignment. Eur Spine J [Internet]. 2016;
24. Jeon C-H, Lee H-D, Lee Y-S, Seo H-S, Chung N-S. Change in Sagittal Profiles After Decompressive Laminectomy in Patients With Lumbar Spinal Canal Stenosis. Spine (Phila Pa 1976) [Internet]. 2015;40(5):E279–85.
25. Lim JK, Kim SM. Comparison of Sagittal Spinopelvic Alignment between Lumbar Degenerative Spondylolisthesis and Degenerative Spinal Stenosis. J Korean Neurosurg Soc [Internet]. 2014 Jun;55(6):331–6.
26. Suzuki H, Endo K, Kobayashi H, Tanaka H, Yamamoto K. Total sagittal spinal alignment in patients with lumbar canal stenosis accompanied by intermittent claudication. Spine (Phila Pa 1976) [Internet]. 2010 Apr 20;35(9):E344–6.
27. Fujii K, Kawamura N, Ikegami M, Niitsuma G, Kunogi J. Radiological Improvements in Global Sagittal Alignment after Lumbar Decompression without Fusion. Spine (Phila Pa 1976) [Internet]. 2015;40:703–9.
28. Hikata T, Watanabe K, Fujita N, Iwanami A, Hosogane N, Ishii K, et al. Impact of sagittal spinopelvic alignment on clinical outcomes after decompression surgery for lumbar spinal canal stenosis without coronal imbalance. J Neurosurg Spine [Internet]. 2015;23(4):451–8.
29. Been E, Barash A, Marom A, Kramer P a. Vertebral bodies or discs: which contributes more to human-like lumbar lordosis? Clin Orthop Relat Res [Internet]. 2010 Jul [cited 2014 Sep 22];468(7):1822–9.
30. Lafage R, Schwab F, Challier V, Henry JK, Gum J, Smith J, et al. Defining Spino-Pelvic Alignment Thresholds: Should Operative Goals in Adult Spinal Deformity Surgery Account for Age? Spine (Phila Pa 1976) [Internet]. 2016 Jan;41(1):62–8.
31. Diebo BG, Ferrero E, Lafage R, Challier V, Liabaud B, Liu S, et al. Recruitment of compensatory mechanisms in sagittal spinal malalignment is age and regional deformity dependent: a full-standing axis analysis of key radiographical parameters. Spine (Phila Pa 1976) [Internet]. 2015 Feb;40(9):642–9.
32. Akbar M, Terran J, Ames CP, Lafage V, Schwab FJ. Use of Surgimap Spine in Sagittal Plane Analysis, Osteotomy Planning, and Correction Calculation. Neurosurg Clin N Am [Internet]. 2013/04/09 ed. Elsevier Inc; 2013 Apr [cited 2013 Aug 12];24(2):163–72.
33. Lafage R, Ferrero E, Henry JK, Challier V, Diebo B, Liabaud B, et al. Validation of a new computer-assisted tool to measure spino-pelvic parameters. Spine J [Internet]. 2015 Sep 4;
| How to Cite this Article:Diebo BG, Varghese JJ, Schwab FJ. Factors Influencing Sagittal Malalignment and its effect on Clinical Implications in Adult Spinal Deformity. International Journal of Spine Apr – June 2016;1(1):5-9. |

(Abstract) (Full Text HTML) (Download PDF)
Post-operative Extensively Drug Resistant Mycobacterium Tuberculous Discitis
Volume 1 | Issue 1 | Apr – June 2016 | Page 47-49|Dhiraj Vithal Sonawane[1], Eknath Pawar[2], Ajay S Chandanwale[3],Ambarish A Mathesul[3], Abhishek Salunke[4], Swapnil M Keny[1].
Authors :Dhiraj Vithal Sonawane[1], Eknath Pawar[2], Ajay S Chandanwale[3],Ambarish A Mathesul[3], Abhishek Salunke[4], Swapnil M Keny[1]
[1] Department of Orthopaedics, Grant Medical college, & Gokuldas Tejpal Hospital, Mumbai
[2] Department Of Orthopaedics, Grant medical college, Mumbai.
[3] Sasoon Hospital & BJMC, Pune
[4] Gujarat Cancer Research Institute
Address of Correspondence
Dr. Dhiraj V. Sonawane
Grant Medical college, & Gokuldas
Tejpal Hospital, Mumbai
Email: dvsortho@gmail.com
Abstract
Mycobacterium tuberculosis (MTB) as a cause of postoperative discitis is extremely rare. We report a first case of extensively drug resistant mycobacterium tuberculosis (XDR-TB) as cause of early postoperative discitis, confirmed on culture and sensitivity. XDR-TB is looming threat and remains a challenge in management .Even with present day available treatment options the prognosis remains poor. Reviewing the literature we discuss possible management in XDR TB discitis.
Introduction
Post-operative discitis is an uncommon but devastating complication after invasive spinal procedure [1, 2]. The incidence of post procedural discitis ranges from 0.26 to 4% [2]. Most common organisms responsible are Staph. aureus and streptococcus species. Three cases of postoperative discitis due to mycobacterium tuberculosis are reported in English literature [3, 4, 5]. XDR TB by WHO global task force on XDR TB, is defined as TB which is resistant to isoniazid and rifampin, plus resistant to any fluoroquinolone and at least one of three injectable second-line drugs (i.e., amikacin, kanamycin, or capreomycin). XDR-TB & TDR-TB (totally drug resistant tuberculosis) continues to pose challenge to control program and treating physician [6, 7, 8, 11]). We report 1st case of XDR TB discitis and discuss possible therapeutic options.
Case report:
A 61 year old male, known case of diabetes and hypertension was operated with laminectomy and discectomy for L3-4 disc prolapse in December 2010 (Fig 1a, b).
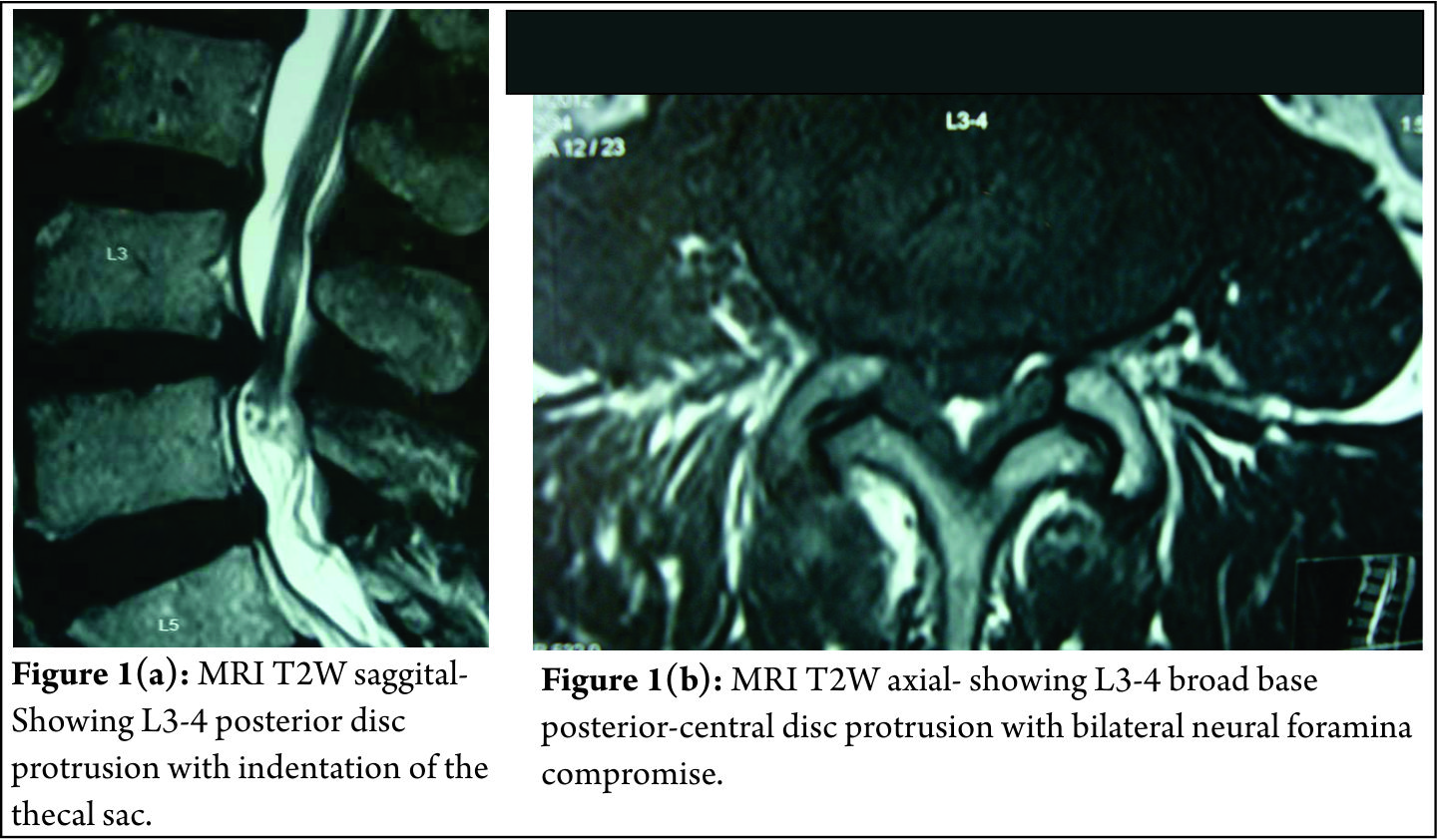
Pre operatively patient had left ankle dorsiflexion MRC grade 3 and depressed left knee reflex. Neurological status remained same after surgery. Three weeks after surgery, patient developed seropurulent discharge through the operated wound. Erythema and induration was present on upper end of wound. Hematological investigation showed TLC- 17,000/ cmm, ESR- 48 mm at end of one hour and CRP 4 mg/dl. Pus culture of discharge grew Pseudomonas aeruginosa. Antibiotics were given according to sensitivity for a period of 4 months, but discharge through the wound continued. Plain radiographs 4 months after surgery showed destruction of L3-4 vertebral end plates with lumbar kyphosis (Fig. 2a). MRI demonstrated altered marrow signal in L3, 4, 5 vertebral bodies with epidural soft tissue causing compression of dural sac, suggesting L3-4 infective spondylodiscitis (Fig 2b). Surgical debridement was done. Intra operative sample from disc space revealed acid fast bacilli on staining. On retrospective evaluation, patient had no past or family history of tuberculosis (TB) or TB contact. X-ray chest was normal. Patient was started on Isoniazid (H) 300mg, Rifampicin (R) 450mg, Ethambutol (E) 600mg & Pyrazinamide (Z) 750mg daily. BACTEC report at 4 weeks showed mycobacterium tuberculosis resistant to all the 1st and most of 2nd line anti tuberculosis drugs (ATT) including ciprofloxacin and kanamycin but sensitive to Amikacin and Clarithromycin. Four drug ATT was discontinued. Patient was started on PZA, Levofloxacin, cycloserine, and Amikacin as per advice of TB physician. After 2 weeks, discharging sinuses with pale granulation at the opening developed. Another surgical debridement with interbody fusion (cage and bone grafting) and posterior stabilization was done (Fig 2c). However, patient’s condition did not improve. ESR (68mm/hour) and CRP (5.8 mg/dl) remained elevated. Because of the rising serum creatinine level (2.5 mg %), Amikacin was discontinued. The follow up radiograph at 1 month post surgery showed vertebral destruction with implant loosening and progression of the kyphotic deformity (Fig. 3). Eighty eighth day postoperatively, patient status deteriorated suddenly and he developed sudden altered sensorium and neck stiffness. He was intubated and kept on vertilatory support, however his condition kept on deteriorating and he died on ninety first postoperative day. The suspected cause of death was meningitis. No Autopsy was performed.
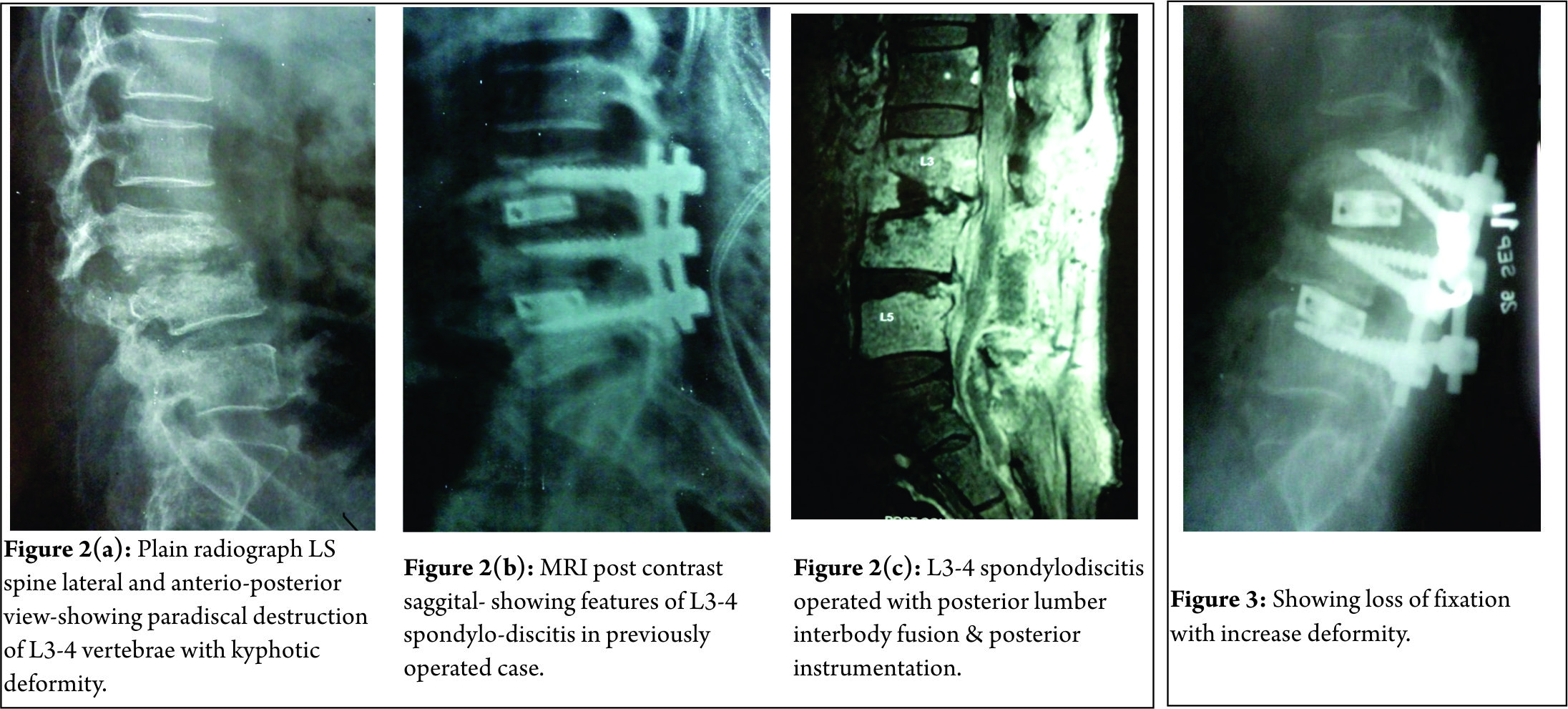
Discussion:
The incidence of post-operative discitis is 0.7 to 0.8 % after antibiotic prophylaxis [1,2]. Discitis results due to haematogenous spread in pediatric age group and by direct inoculation in adults [2]. In TB it possibly spreads from adjacent involved urinary tract [3]. The common organisms are staph. aureus, strep. species, and anaerobic organisms. Other rare organism includes, Mycobacterium tuberculosis (MTB), Candida albicans, Mycobacterium cheloni, Propionibacterium acne [2,3]. The risk factors associated are diabetes, malnutrition, smoking, obesity, alcohol abuse and instrumentation. Early post-operative infection usually presents as wound dehiscence and discharge within 3months of surgery, while late post-operative infection may present within 7 years of surgery with milder symptoms. MRI with contrast enhancement is modality of choice with specificity (93%) and sensitivity (96%) for detection of vertebral infection. [2, 3] In recent years because of use of broad spectrum antibiotics and increased number of people with immunocompromised status there is rise in infections secondary to unusual organisms like MTB [12].On literature search, we found 3 reported cases of post-operative discitis due to M.TB [3,4,5]. Jeon DW et al [4] reported a case of post L4-5 discectomy, MTB spondylodiscitis with bizarre course. MRI showed feature of spondylodiscitis. The biopsy sample was positive for TB PCR specific for MTB. Patient was managed with curettage and interbody fusion using autologous iliac bone grafting and antituberculous therapy (ATT). Patient showed successful fusion and clinical improvement. Iraj lotfinia et al [3] reported similar case of post L4-5 discectomy due to MTB. Patient was managed conservatively with HRZE for 2 months and HR for 10 months, with good outcome. Kaplan ES [5]reported a case of post L4-5 discectomy tuberculous abscess, successfully treated with 3 drugs ATT.
The management for post-operative discitis is conservative approach with organism specific antibiotics and bracing. Those patients who fail to respond to above treatment, with continued pain, infection, spinal deformity require an operative intervention consisting of anterior debridement and interbody fusion with autologous bonegraft and posterior stabilization.
The available treatment options for XDR-TB includes use of later generation fluoroquinolone (levofloxacin, moxifloxacin, sparfloxacin) plus addition of likely active drugs (MTB strain susceptible to drugs tested and drugs to which patients had not been previously exposed) plus linezolid [10]. Surgery will help in taking specimen for diagnosis, reducing bacterial load by debridement, with advantage of fusion. In our case, because of the resistant nature of organism and limited therapeutic options the disease progressed and treatment failed. Meta analytic study using later generation cephalosporins, likely active drugs, linezolid and surgery in pulmonary XDR-TB showed a favourable outcome of 43.7% with death of 20.8% patients [10]. The newer drugs in XDR-TB are less effective, more toxic, and costlier [9, 11]. Therefore further research in development of better anti-tuberculosis drugs (ATT) is required.
References
1. Anthony E. Harris, Chrisanne Hennicke, Karin Byers, William C. Welch. Postoperative discitis due to Propionibacterium acnes: a case report and review of the literature . Surgical Neurology 63 2005; 538–541.
2. Jeff S. Silber, Greg Anderson, Alexander R. Vaccaro, Paul A. Anderson, Paul McCormick. Management of postprocedural discitis. The Spine Journal. 2002; 2:279–287.
3. Iraj Lotfinia , Payman Vahedi . Late-onset post-diskectomy tuberculosis at the same operated lumbar level: case report and review of literature . Eur Spine J 2010;19 (Suppl 2):226–232 .
4. Jeon do W, Chang BS, Jeung UO, Lee SJ, Lee CK, Kim MS, Nam WD. A case of postoperative tuberculous spondylitis with a bizarre course. Clin Orthop Surg. 2009 Mar;1(1):58-62..
5. Kaplan ES .Post-diskectomy tuberculous abscess. J Neurosurg 1973;38:358–361.
6. World Health Organization. Multidrug and extensively drug-resistant TB (M/XDR-TB): 2010 Global report on surveillance and response. 2010. Available at: http://www.who.int/tb/publications/2010/978924599191/en/ Accessed 25 Nov 2010.
7. World Health Organization. Guidelines for the programmatic management of drug-resistant tuberculosis. Emergency update 2008. 2008. Available at: http://www.who.int/tb/publications/2008/programmatic_guidelines_for_mdrtb/en/index.html Accessed 25 Nov 2010.
8. World Health Organization. Global tuberculosis control: a short update to the 2009 report. Available at: http://www.who.int/tb/publications/ global_report/2009/update/en/ Accessed 25 Nov 2010.
9. João Alves de Araújo-Filho, Arioldo Carvalho Vasconcelos-Jr, Eduardo Martins de Sousa, Colombina da Silveira, Elisangela Ribeiro, André Kipnis et al . Extensively Drug-Resistant Tuberculosis: A Case Report and Literature Review . BJID 2008; 12: 447- 452 .
10. Karen R. Jacobson, Dylan B. Tierney, Christie Y. Jeon, Carole D. Mitnick, Megan B. Murray. Treatment Outcomes among Patients with Extensively Drug-Resistant Tuberculosis:Systematic Review and Meta-Analysis . Clinical Infectious Diseases 2010; 51(1):6–14
11. Chee Kiang Phua, , Cynthia BE Chee, Angeline PG Chua, Suay Hong Gan, Aneez DB Ahmed, Yee Tang Wang . Managing a Case of Extensively Drug-Resistant (XDR) Pulmonary Tuberculosis in Singapore . Ann Acad Med Singapore 2011;40:132-5 .
12. Sapkas GS, Mavrogenis AF, Mastrokalos DS, Papadopoulos E, Papagelopoulos EC, Papagelopoulos PJ (2006) Postoperative spine infection: a retrospective analysis of 21 patients. Eur J Orthop Surg Traumatol 16(4):322–326.
| How to Cite this Article: Sonawane DV, Pawar E, Chandanwale A, Mathesul AA, Salunke A, Keny SM. Post-Operative Extensively Drug Resistant Mycobacterium Tuberculous Discitis. International Journal of Spine Apr – June 2016;1(1):47-49 . |