
Thoracolumbar Spinal Injuries – Evolution of Understanding of fracture Mechanics and Management Options
Volume 1 | Issue 2 | Sep – Dec 2016 | Page 7-8 | Shailesh Hadgaonkar, Ketan Khurjekar
Authors : Shailesh Hadgaonkar [1], Ketan Khurjekar [1]
[1] Sancheti Institute for Orthopaedics &Rehabilitation, Pune, India.
Address of Correspondence
Dr Shailesh Hadgaonkar
Sancheti Institute for Orthopaedics &Rehabilitation, Pune, India
Email: editor.ijspine@gmail.com
Introduction
This symposia on thoracolumbar fractures is aimed at providing an overview to the reader with respect to evolving trends in fracture diagnosis and management.
There has always been controversies in treating thoracolumbar spine injuries with neurological deficit, but as we know the goal of managing these T-L junction injuries is to maintain the sagittal alignment for mechanical stability and to give additional support for rehab and physiotherapy for neurological recovery. The main aim of thoracolumbar fracture surgery is to give structural support to the spinal column for wheelchair mobilization in cases with complete injury and paraplegia. We have found significant improvement in quality of life in patients who were operated for these severe thoraco lumbar spinal injuries. As we all know the most common level of these injuries is T 12 and L1, sustaining from the high velocity trauma. The flexibility at thoraco lumbar junction, the thoracic rib cage ending at the junctional level, coronal alignment of facet joint in thoracic spine and the changes in the lower thoracic facets to less coronal alignment is likely to cause fracture dislocations. Various transitional zone injuries- between T 11- L2 are approximately 50 – 60 % of all injuries. Most common reason for these injuries – are fall from height and high velocity RTA. There is a significant association of other injuries such as chest, abdominal, vascular injuries and also head injuries with these fracture dislocations.
It is paramount to evaluate these patients in detail, thorough clinical and neurological assessment is mandatory. The standard American Spinal Injury Association (ASIA) guidelines should be followed in neurological assessment. Associated relevant investigations as the X-rays and MRI scans will guide for non-operative Vs operative management. Additional modalities such as CT scans and 3D reconstruction is important clinically unstable and high grade T-L injuries. Primary assessment and medical management is important to stabilize the patient before planning the surgery.
Evolution of classification systems :
Various different classification system have evolved from the World War I and II days, as Bohler in 1930 classified T-L fractures into five categories :-
1- Compression fractures
2- Flexion /distraction injuries
3- Extension fractures
4- Rotational injuries
5- Shear fractures
Watson Jones in 1938 classified T-L injuries adding instability to Bohler’s classification. The most important factor in Watson Jones classification was description of Posterior ligamentous complex (PLC) in spine stability, as they felt the integrity of interspinous ligament is most important stability factor.
Nicole in 1949, further classified using anatomical classification with emphasis on interspinous ligament integrity. He described the stability structures as the vertebral body, disc, intervertebral joint, and interspinous ligament. This classification serves as a foundation for subsequent classifications.
Holdsworth in 1963, described Two column theory and he emphasized the spinal stability on posterior ligamentous complex (PLC) stability. Kelly and Whitesides attempted to modify Holdsworth classification, as they specifically mentioned anterior column as solid vertebral body whereas posterior column as posterior elements and neural arch. Also they emphasized the treatment of neurological deficit.
Dennis in 1983, came up with a new concept – Three column theory using the radiological parameters. He provided a new insight in detailing the classification into anterior, middle and posterior column. They described the middle column – osteo-ligamentous complex injury is the primary determinant of mechanical spinal stability.
Mcafee et al described the classification based on CT scans of 100 consecutive patients and divided into 6 groups. This was the most detailed classification system in the 1980’s. They described the height loss of vertebral body, facetal joint subluxation, fragments in the spinal canal, progressive neurological deficit, kyphosis angle because of instability was assessed with the CT scan. As per their criteria translational and flexion/rotational fracture dislocation and posterior ligamentous complex (PLC) injury with kyphosis more than 30 degrees angle should undergo surgery.
In 1994 Mc Cormack classified on load sharing concept, which focuses more on location of the fracture in the vertebral body.
Then in 1994, Magrel et al came up with classification based on evaluation of 1445 cases and classified into 3 types and 53 injury models.
In 2005, Vaccero et al came up with Spine trauma study group – Thoraco Lumbar Injury Classification System (TLICS) which takes a detail note on fracture mechanism, the intact PLC status and the neurological status of the patient.
TLICS points:
Fracture Mechanism
Compression fracture 1
Burst fracture 1
Rotational fracture 3
Splitting 4
Neurological involvement
None 0
Nerve root 2
Medulla spinalis, conus medularis-
– Incomplete 3
– Complete 2
Cauda equina 3
Posterior ligamentous complex
Intact 0
Possibly injured 2
Injured 3
Surgical indication is for cases with 5 points or more, cases with 4 points are between surgical vs non surgical, and cases with 3 or less points are non surgical. It is quite a comprehensive and popular classification in clinical practice and many centers prefer to use this classification worldwide.
Recently AO Spine knowledge forum has proposed a comprehensive modified AO classification based on morphology of fracture, neurology status and description of relevant patient specific modifiers
These classifications signify the growth in our understanding of pahtomechanics of the spine fracture as well as takes into account our growing expertise in the offering better surgical options to the patients.
Management Options:
Various management options are discussed in the current symposia and most of the options are individualised depending on the etiology and extent of fracture. Few general rules are noted below –
– Cases where there is retropulsion up to 40- 50 degrees without neurological deficit with intact PLC we can attempt indirect decompression and distraction in first 5 -6 days after the injury.
– Cases with less angulation and wedging with minimal kyphosis can be dealt with short segment fixation.
– Interlink in long construct always adds-up to the stability. Reduction of the dislocation with various maneuvers always beneficial for sagittal profile.
– Role of steroid is controversial post T-L injury with neurological deficit and is rarely used worldwide.
– Role of minimally invasive spine (MIS) surgery is evolving and needs a longer follow up. MIS surgery helps in reducing the bleeding, morbidity in selective cases.
– There is a significant role of rehabilitation post-surgery, in cases of T-L fractures with neurological deficit. Stem cells are promising in animal and Fish models in research labs and we are very hopeful about the same in humans.
Most of the above options are discussed in details in the symposia and we would encourage the readers to go through the articles. Ultimately the clinical evaluation summed with the radiological parameters will decide the management plan as cases with instability, neurological deficit and progressive neurological worsening cases will need surgical intervention. A lot of cases can be conserved with careful monitoring.
We thank all the authors and contributors for participating in the symposia and invite interested readers to participate as symposium editors or authors. Please write to us by email and provide your suggestions and comments.
| How to Cite this Article: Hadgaonkar S, Khurjekar K. Thoracolumbar Spinal Injuries Evolution of Understanding Fracture Mechanics and Management Options . International Journal of Spine Sep-Dec 2016;1(2):7-8. |

(Abstract) (Full Text HTML) (Download PDF)
Interview with Dr Rajasekaran: Part I
Volume 1 | Issue 2 | Sep – Dec 2016 | Page 3-6 | Prof. S. Rajasekaran
Authors : Prof. S. Rajasekaran
M.S., DNB., F.R.C.S.(Ed)., M.Ch(Liv)., FACS., F.R.C.S.(Eng)., Ph.D
Chairman, Dept of Orthopaedics, Trauma & Spine Surgery.
Ganga Hospital, Coimbatore.
Prof. S Rajasekaran
One of the most Revered Academicians and most decorated Spine surgeon in India, Dr Rajasekaran has inspired an entire generation of Orthopaedic Surgeons across the country. This interview is an attempt to gain an insight into Dr Rajasekaran as a human being as an academician and as an Orthopaedic Surgeon
This interview with Dr S Rajasekaran (SR) was conducted at Kochi at the venue of IOACON 2016. The interview was conducted by Dr Ketan Khurjekar (KK) and Dr Ashok Shyam (AKS). The purpose of this interview was to know more about the journey of Dr Rajasekaran and also to catch a glimpse of his life and personality. A broader objective is to attract people to excellence in orthopaedics and to have pride in our own people who have done exceptionally well in reaching international acclaim in respective fields. This is part I of the interview and part II will be published in the forthcoming issue.

KK: Today you are at cross roads or rather in middle of world orthopaedic landscape and have experienced so many things. You were the IOA president and know about the national scenario and you are now involved in many international association including SICOT, SRS and AO spine. You are exposed to working in India as well as the western world. What are the differences that you perceive between the two worlds and how can we can attain the next level especially in terms of western world?
SR: Successful persons worldwide share the common trait of being focussed and hardworking. Indians as a rule, we work hard (may be even harder than the west) but the western world works with more focus and planning. We work hard and grow but they plan ahead and work towards the goals. Our growth is a more like an organic growth. We all are better than what we were 10 years ago but most of our growth is unplanned. When you don’t have a planned and targeted growth, you often don’t achieve or reach your greatest potential. For example, say a department did 1000 surgeries a year and 1100 the following year. This represents a growth of 10% and one can be happy about it. But the other way of looking at it is if the growth could have been up to 2000 surgeries? To achieve this type of growth, planning in advance is essential. Once a realistic goals have been set, timely audit, at least every every 3 months and a critical appraisal of performance will help to achieve the targets. Otherwise, performance deficit is common.
We have to realise that time waits for no body and keeps on moving. All of us have only a certain amount of time and certain of amount energy and this has to be channelised and not wasted. So we have to have concentrate our time and energy towards our targets. When you are doing things that you don’t need to do, then there is very little time to do what you really want to do. Every activity that is undertaken that is not in line with the long or short term plan, actually amounts to distraction. So we have to learn to say ‘No’ to things that waste our time.
Goals also have to be very specific rather than vague. Every new year, probably most of us aim to be better surgeons and to do more surgeries. But these will be the goals of every orthopaedic surgeon and is very nonspecific, without concrete plans or strategies. Plans need to be specific, time bound, realistic and tangible. And this makes a very huge difference.
Growth is either organic or planned. Orthopaedic speciality in India is growing by 15 to 18% every year. If one is growing at rate of 15%, you can’t take pride in that as you are riding the general growth of the speciality. So unless the growth is by more than 10% of the general growth we cannot take credit for it. If you are growing less than the national average, then someone else is growing much faster than you. So to be aware of one’s growth and performance in relation to other people around you is important.
It is also important not to assess just the performance but also the ‘performance gap’. Not appreciate ourselves on the performance that we have achieved but look at the highest possible that we could have performed and note if we have achieved it. Most of us our very happy in patting ourselves too easily and very early. This can be a big problem. I think achievers are more tuned toward looking at the performance gap and improving themselves continuously.
AKS: Does that mean we should be a bit discontent?
SR: We should have clarity on this subject. Contentment of mind is something that is spiritual and is needed for your happiness, peace of mind and healthy living. But contentment is a poisonous word when it comes to your work and professional life. People often confuse contentment in life and contentment in professional work. When the elders advocate contentment, they simply mean not to be greedy in life. They didn’t advocate to perform less or be happy with poor performance. Contentment is a good word for your spirit but not so good for your work. We should be contended only in worldly possessions but as far as the excellence in academics and profession is concerned, ‘passion for more’ is necessary. I would say you should have fire in your belly every day in your profession. At any time there is a reduction in passion for excellence, there is going to be stagnation.
KK: How then do we achieve our fullest ability?
SR: I often quote the famous words of Dr APJ Kalam, “Small aim is a crime”. One has to aim to achieve to his fullest capacity, whatever that may be. For this to happen, people with whom you spend time and interact become very important. I am often asked the advantage of being closely involved in international societies and also playing leadership roles in them. The most important benefit, and which I really enjoy is the ability and opportunity to move shoulder to shoulder with other giants in the field. I think this is really true – ‘you are the sum average of the five people you constantly move with’. This is very very important. If you are always interacting with people who are high thinking and who are professionally oriented and who are high achievers, you will be motivated towards higher performance than before. In contrast if one spends time with people who are distracted or poor achievers there is every chance that your performance will come down too. So one’s concept of hard work, happiness, contentment, definition of good life is all defined by people with whom you move with, people whom you look up to and people who look up to you.
There is a saying ‘If you are the best person in the room, then you are in the wrong room’. You have to move to a room where there are better persons than you. If you work with better people than you, then it becomes an incentive to improve your life. So it is vital to choose colleagues and friends who are better than you. It will keep you humble and help you to raise your bar from time to time. This is very important.
KK: We have seen that you are not easily attracted to material positions like luxury cars. I always wonder about this?
SR: At different periods of time in your life, different things impress you and it’s probably a sign of growing up. I was really impressed with jaguar cars when I was in England, specially the olive green car XJ8 model. I have taken many pictures of them with me standing in front of the car. My wife was really tired with this and told me to buy one and get over my obsession with it. I could not afford it at that time and I think that the attraction was increased by my inability to buy the car. That really made the car more attractive. At this stage of life where I can buy any car easily, the attraction has just simply vanished. So one gets over your attractions as you grow up . Your focus in life changes.
Please don’t get me wrong. I am not against worldly pleasures or luxury cars etc. I do love a ‘good life’ and I think that we should indulge ourselves from time to time. Life should not be just a bed of nails and should be sprinkled with worldly pleasures also. But not to a point of distraction. We need to keep the proportion and balance. Sometimes we have to get a luxury car to know that it is the most important thing in life. Sometimes they look more important than what they are until they are acquired. Happiness is basically a personal issue. Does not depend on your worldly possessions. If you are sad, having a BMW does not change things in any way. If you have had a successful day, it doesn’t make any difference whether you are travelling in an ambassador or BMW, you will still feel happy.
Materialistic indulgences from time to time is also important. Don’t need to be a ‘sanysi’ to be an achiever. It is the enthusiasm, inquisitiveness and the energy to do things that is very important.
KK : What is your opinion about hard work and professional stress?
SR: This is another area where there is a lot of confusion amongst the younger generation.
Hard work is completely different and has nothing to do with stress. Hard work is important as it allows you to achieve your dreams and give you professional satisfaction which are very important for happiness. Hard work is necessary for success and you can never be happy if you are unsuccessful in your profession. Productive hard work has never harmed anybody. In fact if we look back in our lives, we always remember fondly the times that we have worked hard and achieved a lot. Every surgeon feels happy when he has more work than less. All of us have to accept that.
But stress is something completely different and has to be avoided. It comes from a variety of factors like poor performance and failures in day to day work. Very frequently the cause of stress is lack of hard work, poor preparation and under performance. Stress also comes from doing a work which you are not passionate about. Stress is not working 15 hours at a job you like. Stress is working even 15 minutes at a job you dislike. a. If you are not passionate about your profession and you are feeling stressed you must look seriously at alternatives. Stress can also come from work place problems, incompatibility with working colleagues and family members, uncontrolled anger, jealousy etc. These issues are more relevant and are cause for poor health than hard work. The reason why worry kills more people than work is that nowadays more people worry than work.

In my experience, the most happiest people are the people who are fortunate enough to love what they do and be able to do what they love. They don’t need any further incentive for performing well.
Lastly, it is important to have a ‘wholesome life’. We need some buffers in life and best one is a loving and happy family. If you are struggling in family life, you would be pretty stressed in every area of life. A happy family is probably the most important factor and one needs a good ‘work – life balance’.
– To be continued in Next Issue of IJS
Dr S Rajasekaran
M.S., D.N.B, F.R.C.S(Ed)., F.R.C.S.(Lond))., M.Ch. , FACS, Ph.D.
Dr Rajasekaran is the Chairman of the Department of Orthopaedics & Spine Surgery, Ganga Hospital, Coimbatore, India and Adjunct Professor of Orthopaedic Surgery, The Tamilnadu Medical University.
Dr Rajasekaran holds several administrative and academic positions in Spine Surgery. He is the Current President of the Association of Spine Surgeons of India, President Elect of Indian Orthopaedic Association, President of the World Orthopaedic Concern, UK, President of Computer Assisted Orthopaedic Surgery Society, India, and Founder Chairman of Trauma Section of Asia Pacific Orthopaedic Association. He has also been elected as the Hunterian Professor 2011-12 by the Royal College of Surgeons of England.
Dr Rajasekaran heads one of the largest clinical and research units in Spine Surgery in South Asia. His research interests relate to disc biology and nutrition, Diffusion Tensor Imaging of the Spinal Cord, Genetic basis of disc degeneration and kyphotic deformities in spinal tuberculosis on which he has 151 publications in international journals. He has authored many chapters in Textbooks and is the Chief Editor of a Video Atlas in Spine Surgery and Chief Editor of ASSI Textbook of Spinal Infections & Trauma.
Dr Rajasekaran is the Deputy Editor, SPINE, USA and serves as a Editorial Board Member of European Spine Journal, Journal of Craniovertebral Surgery and Journal of Orthopaedic Science, Japan. He is the recipient of many awards in spine research which include the ISSLS Award for 2004 & 2010, EuroSpine Open Paper Award in 2008, APOA Award in 2007 and Sofamer Danek Award of ISSLS for the years 1996, 2002 and 2006.
| How to Cite this Article: Rajasekaran S. Interview with Dr Rajasekaran: Part I. International Journal of Spine Sep-Dec 2016;1(2):3-6. |
 Prof. S. Rajasekaran |
(Abstract) (Full Text HTML) (Download PDF)
Management of Pathological vertebral collapse in elderly
Volume 1 | Issue 2 | Sep – Dec 2016 | Page 22-26 | Rajesh Parasnis, Alpesh Thumbadiya, Sachin Pathak, Shantanu Patil
Authors : Rajesh Parasnis [1], Alpesh Thumbadiya [1], Sachin Pathak [1], Shantanu Patil [1]
[1] Oyster and pearl hospital, Pune
[2] Jehangir Hospital, Pune
[3] SRM Medical College, SRM University, Kattankulathur, Tamil Nadu 603203
Address of Correspondence
Dr. Rajesh Parasnis
Department of Spine Surgery, Oyster and pearl hospital, India.
Email : rajeshparasnis@rediffmail.com
Abstract
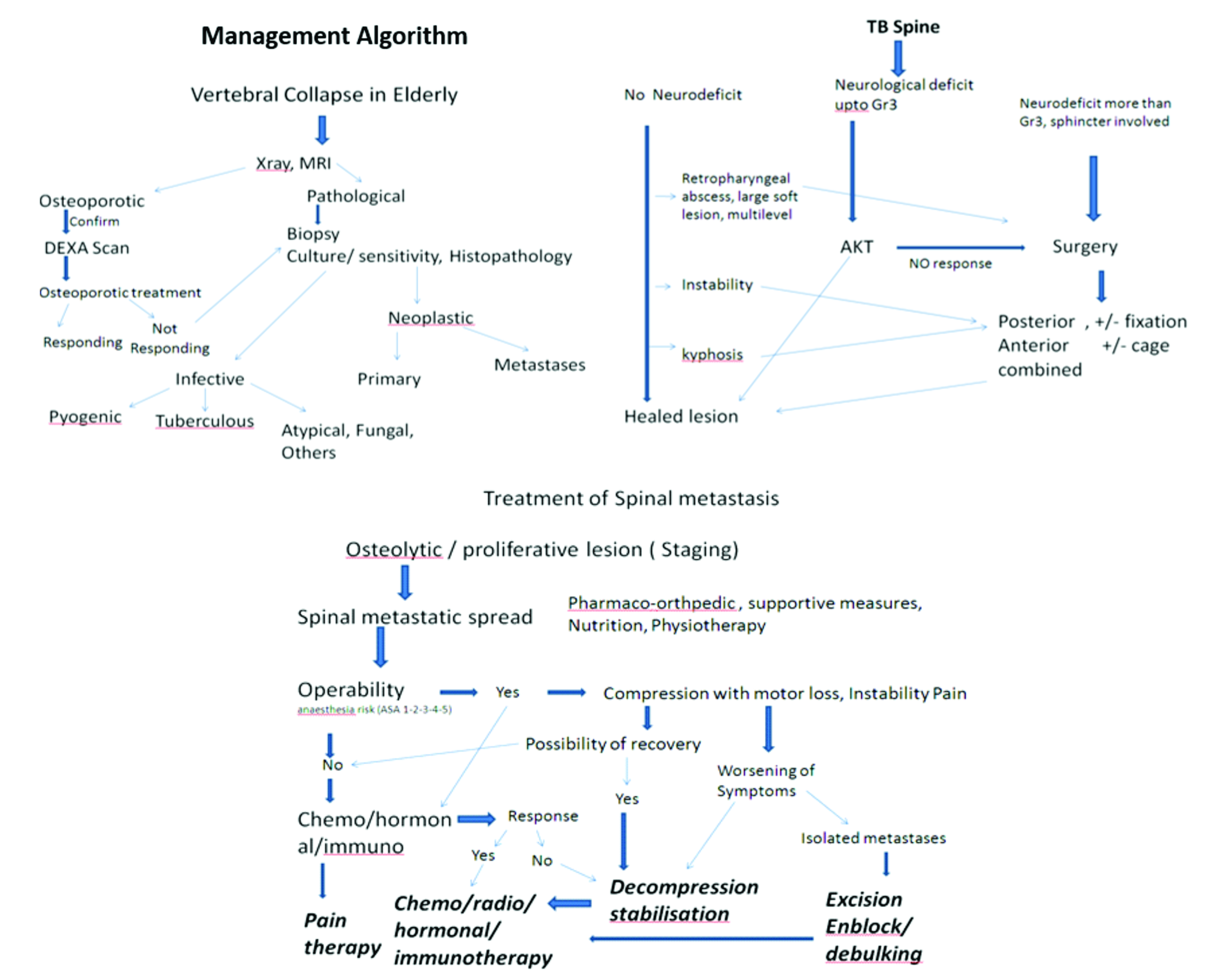
Pathological vertebral fractures can be due to various reasons and management plans will differ as per the diagnosis. We present our series of patient with pathological fractures along with a management algorithm
Material and Methods: All patients aged more than 60 years presenting with intractable back pain with or without neurological deficit were screened. Of the 532 patients, 274 osteoporotic insufficiency fractures were identified by DEXA scan and excluded from the analysis. 258 patients with vertebral collapse caused by infection or neoplastic conditions were included in study.
Results: 212 patients (82.2%) had a single vertebral lesion followed by 34 (13.2%) at 2 levels and 12 (4.7%) with multiple vertebral levels involved. 161 cases (62.9%) had an infective pathology while the remaining 97 (37.9%) had a neoplastic cause. Needle biopsy was positive in 218 (84.49% ) cases. Repeat biopsy was required in 39 cases where Fine Needle Aspiration Cytology (FNAC) was inconclusive. There were 130 tubercular lesion, 7 atypical tuberculosis, 5 MDR tuberculosis, 13 pyogenic, 2 fungal, 4 hydatid cyst, 24 malignant lesions and 73 metastasis. 60 patients (58 TB spine and 2 pyogenic infection) were managed without surgery and the remainder 197 patients underwent surgical intervention
Conclusion: Pathological fractures can be due to varied etiology and although tuberculosis formed major cohort in our series, neoplastic lesion had to be suspected and tissue biopsy is essential to reach correct diagnosis and management plan
Keywords: Thoracolumbar fractures, pathological fractures, biopsy.
Introduction
Atraumatic vertebral collapse is a common clinical problem, especially in elderly population (1). It includes fractures because of osteoporosis or any other pathological cause. Pathological vertebral fracture in elderly occurs due to infective or neoplastic condition. Spinal column affection by neoplastic lesions include primary (benign or malignant ) or secondary metastasis. 50 to 85% of patients with cancer experience skeletal metastasis, most commonly in the spine (2). Infection of spine occurs due to tuberculosis, atypical tuberculosis, pyogenic, fungal and parasitic infestation (e.g.hydatid cyst). Tuberculosis is most common among them and a major health problem in developing countries. In elderly population because of comorbidity and lower immunity, spinal affection by tuberculosis is high.
The spine has a load-bearing and a neuro-protective function, Any failure of its structural integrity as a result of metastatic or infective vertebral involvement often brings about severe pain and/or paralysis. These symptoms impair the ambulatory ability of the patients and worsen their quality of life. One of the main causes of severe pain or paralysis is pathologic vertebral body collapse caused by an osteolytic lesion. Therefore, prevention and treatment of collapse is a key factor in maintaining the patients’ ambulatory ability especially in morbid elderly population (3,4,5,6). Early diagnosis of such conditions is very important to start with proper treatment.
Diagnosis of pathological vertebral collapse in aged population is usually missed or delayed. Elderly patients presenting with backache and vertebral collapse are a challenge for diagnosis as well as for management. Correct diagnosis may require all blood invastigations and imaging modalities including plain X-rays, ultrasonography (USG), computed tomography (CT), radionuclide bone scan, magnetic resonance imaging (MRI) and PET scan. For conclusive diagnosis one needs to identify the causative organism and know histopathology of the lesion by biopsy. One may need to repeat the biopsy if required before starting any treatment. It is mandatory to do a culture and test the sensitivity to rule out drug resistance in case of spinal tuberculosis. Management depends on multiple factors and requires multidisciplinary approach.
While many studies have investigated osteoporotic vertebral collapse in the elderly, not many have reported on other pathological fractures. We present our series of such patients and propose a treatment and management algorithm.
Methods and Materials
All patients aged more than 60 years presenting with intractable back pain with or without neurological deficit were identified from a data base spanning seven and half years (May 2008 to Nov 2015 ) at a tertiary care hospital. Of the 532 patients, 274 osteoporotic insufficiency fractures were identified by DEXA scan and excluded from the analysis. 258 patients with vertebral collapse caused by infection or neoplastic conditions were included in study. The patients were classified according to age, gender, pathology, levels affected, region involved, neurological deficit, type of biopsy and management protocol. Base line haematological tests included haemogram, liver function test (LFT), renal function test (RFT), CRP, ESR and serum electrophoresis studies. Radiological studies included Xrays of the affected region ( anteroposterior & lateral views ) and MRI were done in all cases. CT scan, Bone scan, PET scan and Bone marrow examination were done in indicated cases. Tissue diagnosis was done by biopsy in all cases for histopathology and/or culture sensitivity. Management protocol was decided according to the pathology and severity of the lesions. All patients were followed up at regular intervals 3 months, 6 months, 12 months and yearly follow up after that.
Results
The cohort included 258 patients (Male 156: Female 102) aged between 60 and 82 years age (mean age 63.4 years). 212 patients (82.2%) had a single vertebral lesion followed by 34 (13.2%) at 2 levels and 12 (4.7%) with multiple vertebral levels involved. 161 cases (62.9%) had an infective pathology while the remaining 97 (37.9%) had a neoplastic cause. Out of 258 patients mean aged 63.4 years ( 60-82 years ), we found 156 male and 102 female patients. Level of involvement was found to be single, double and multiple in 212 (82.17%), 34 (13.17%) and 12 (4.65%) cases respectively. Infective pathology was found in 161(62.89%) and neoplastic cause was found in 97(37.89%) cases. Distribution of pathology and level affected are detailed in Table 1.
Out of 258, 234 patients presented with intractable pain[predominant back pain in 198 (76.74%) and predominant extremity pain in 62 (24.03%) patients ] of mean duration8.2 weeks ( 1- 32weeks). 68 (26.35%) patients presented with neuro deficit( Frankel grade B in 3, C in 14 and D in 51 ). Constitutional symptoms were present in 38 (14.72) patients. Spinal deformity was present in 21 cases.
Biopsy: Diagnosis of pathological vertebral fracture in elderly age group is usually delayed but sometimes it may be wrongly diagnosed or even missed. Tissue diagnosis is mandatory in all cases. Needle biopsy using Jamshidi needle was done in all suspicious vertebral pathology. Biopsy material was sent for gram stain, Ziehl-Nielson stain, Pus culture and sensitivity, and histopathological examination. Acid fast bacteria culture was advised in relevant cases ( not responding to treatment and MDR Tb ). Gene expert study ( PCR ) for tuberculosis was done in last 2 years only. Needle biopsy was positive in 218 ( 84.49% ) cases. Repeat biopsy was required in 39 cases where Fine Needle Aspiration Cytology (FNAC) was inconclusive. Core biopsy was done in all these 39 cases using large bore Jamshidi needle and it showed malignancy in 19 cases and tuberculosis in 20 cases. In 11patients who had an unbiopsied vertebral lesion initially as primary lesion was confirmed, and not responding to chemotherapy or radiotherapy, a subsequent vertebral biopsy was done. 5 of these patients were diagnosed to have a tuberculous lesion. 27 vertebral collapse initially thought to be osteoporotic on radiological imaging ( MRI and DEXA ) but not responding to osteoporotic treatment were reevaluated by biopsy and turned out to be Koch’s spine in 21 cases and neoplastic in 6 cases. 17 patients who were put on AKT for Koch’s spine but not responding were reevaluated by biopsy and report turned out to be malignant lesion.
Management
60 patients (58 TB spine and 2 pyogenic infection) were managed without surgery and the remainder 197 patients underwent surgical intervention. Non surgical management comprised of bed rest, analgesics, bracing, anti microbial regimen according to pathogen in case of infective lesions.
The 58 patients of tubercular spondylitis were treated by ATT, 4 drug regimen ( Rifampicin, Isoniazide, Ethambutol, Pyrazinamide ) for 3 months, 3 drugs for 3 months, 2 drugs for 3 months. In 2 cases of pyogenic osteomyelitis culture sensitivity specific antibiotics were given intravenously for 2-3 weeks followed by orally for 6 weeks. CBC, CRP, ESR, LFT and RFT were done at regular interval to modify the dosage in all these old age patients.
In MDR cases second line drug therapy was administered and monitored by the Infectious disease specialist.
101 infective lesions were managed surgically ( 92 primary and 9 revision ).
53 patients of spinal tuberculosis were operated by posterior decompression and fixation. 28 patients underwent surgery by posterolateral extrapleural approach and anteroposterior reconstruction. 13 patients were operated by anterior approach for decompression and reconstruction. 7 patients required a combined surgery and reconstruction by anterior and posterior approaches.
All 97 neoplastic vertebral lesions required surgical intervention. Out of 24 primary malignant lesions 3 (out of 7) solitary plasmacytoma were removed enblock, rest all 21 cases were managed by intralesional removal of tumor mass. Pre operative embolisation was done in all vascular tumors ( Solitar plasmacytoma and spindle cell sarcoma ). 1 multiple myeloma and 2 implant related complications required revision surgery.
Out of 73 metastatic vertebral lesions, Vertebroplasty was done in 29 patients, kyphoplasty was done in 6 cases and surgery was done in 38 cases. En block removal was done in 4 patients while in rest 34 cases intralesional removal of tumor was done. Pre operative embolisation was done in all 38 operated cases. 7 cervical and 9 thoracolumbar lesions were operated by anterior approach, 13 thoracolumbar and lumbar lesions were operated by posterior approach, while 9 cases of thoracolumbar and lumbar lesions were dealt by combination of both anterior as well as posterior approach. All 38 operated cases of vertebral metastases were stabilized by at least 2 levels above and 2 levels below with cementation of involved vertebra in posterior approach and anterior reconstruction using cage with autograft.
Chemotherapy and/or radiotherapy was administered according to neoplastic pathology. Post operatively all malignant cases were put on bisphosphonate therapy.
Complications: 4 out of 197 surgically operated elderly morbid patients died in the perioperative period.
Neurological and / or functional improvement was seen in 185 operated cases. Frankel grade B 3 patients improved to grade C in 1 and grade d in 2 cases. Frankel grade c 14 cases showed no improvement in 3 cases, 9 improved to grade D and 2 improved to grade E. Out of 51 Frankel grade D, 4 patients didn’t show much improvement but 37 fully recovered. Operated Koch’s spine all patients showed neurological improvement.
Mean survival time in primary malignancy cases was 36.2 months, while in metastatic cases it was 14.3 months. 7 patients developed recurrence at same level after mean time of 9 months, out of those 2 patients developed paraplegia.
Discussion
Atraumatic vertebral collapse is a common clinical problem, especially in elderly population (1). Osteoporotic vertebral fracture is the major cause in such elderly population. The prevalence of osteoporotic vertebral fractures varied from about 3% in the age group below 60 to about 19% in the 70+ group in women, and from 7.5% to about 20% in men, with an overall prevalence of 11.8% in women and 13.8% in men (7). Among other causes of pathological collapse in the elderly, infective lesions are also common with neoplastic lesions being on the higher side. A fairly high index of suspicion is necessary when dealing with vertebral collapses in the elderly population.
Infection of spine is still a mojor health issue in developing countries. Poor hygiene, poverty, unawareness, poor ventilation along with that other co-morbidities make elderly individual more prone for the infection especially tubercular in developing countries.
With ageing bony trabeculae becomes weak and osteoporotic vertebral collapse become more prevalent. Because the spine has a load-bearing and a nerve-protecting function, failure of its structural integrity as a result of pathological vertebral involvement often brings about severe pain and/or paralysis. These symptoms impair the ambulatory ability of the patients and worsen their quality of life. One of the main causes of severe pain or paralysis is pathologic vertebral body collapse caused by an osteolytic lesion. Therefore, prevention and treatment of collapse is a key factor in maintaining the patients’ ambulatory ability especially in morbid elderly population (3,4,5,6). So early diagnosis of such conditions is very important to start with proper treatment.
Tan DY et al., studied 58 vertebral collapse out of which he found 36 benign vertebral collapses (20 osteoporotic, 7 post-traumatic, 9 infective) and 22 malignant ones (20 metastatic carcinoma, 2 multiple myeloma). In our study we found Infective pathology in 161 (62.89%) [ 13 pyogenic, 130 tubercular, 7 atypical tubercular, 5 MDR tubercular, 2 fungal, 4 hydatid cyst ] and neoplastic lesions in 97 (37.89%) [ 24 primary malignant ( 13 multiple myeloma, 7 solitary plasmacyetoma, 3 lymphoma, 1 spindle cell sarcoma ) and 73 metastases ].The most frequent spinal metastases (60%) are from breast, lung, or prostate cancer (15).
Any elderly patient presenting with intractable back pain especially at night, weight loss and other constitutional symptoms without any history of trivial injury then think of pathological vertebral lesion. Any vertebral collapse detected on a radiograph must initially undergo MRI and routine blood investigations, followed by a DEXA scan to rule out osteoporosis. Even though DEXA scan is indicating osteoporosis it doesn’t always rule out infection or malignancy. In our study we found 27 patients with osteoporotic vertebral collapse, who didn’t respond to osteoporotic treatment and later on confirmed by biopsy as malignancy in 6 cases and infection in 21 cases.
Typical spinal tuberculosis affects the continuous vertebral levels and causes narrowing of the adjacent disc space and bone destruction (8). However, Atypical tuberculous spondylitis shows spondylitis without discitis, isolated central lesion in single vertebral body, non-contiguous skip vertebral body lesions, isolated posterior vertebral elements involvement and isolated intraspinal canal lesions. Atypical form of spinal tuberculosis is difficult to distinguish from malignancy, leading to misdiagnosis and inadequate treatment. Pyogenic and fungal spondylitis, sarcoidosis, metastasis and lymphoma are the close differential diagnosis for tuberculous spondylitis (10, 11).
Differentiating tuberculous spondylitis from these conditions is very important since the line of management completely differs and also early intervention helps in minimizing the residual spinal deformity and permanent neurological deficits (12). Tan DY et al. stated that features which pointed to malignant cause were hypointense marrow on T1-weighted images, marrow enhancement after intravenous contrast, greater than 50% marrow involvement and involvement of posterior elements. Of the vertebral collapses due to infection, 78% showed end-plate disruption(14). Image guided biopsy is very helpful for early diagnosis and prompt intervention if the clinical and imaging findings are not very helpful arriving diagnosis, especially with the atypical presentations (13).
Biopsy: Diagnosis of pathological vertebral fracture in elderly age group is usually delayed but sometimes it may be wrongly diagnosed or even missed. Tissue diagnosis is mandatory in all cases. Needle biopsy is the procedure of choice in definitive diagnosis of pathologic lesions of the spine (17). Needle biopsy is positive in 65% for lytic lesions, incisional biopsy is useful in 85% of blastic lesion while excisional biopsy is positive in >85% for posterior lesions and benign tumors. The percentage of positive results of biopsy are higher in metastases than primary tumors. The cystic and sclerotic vertebral tumors have less positive results. Transpedicular biopsy with Jamshidi needle has better success rate than FNAB in such lesions.
Once tissue diagnosis is done by biopsy then one should go ahead with other investigations such as CRP, ESR, Procalcitonin for infective pathology. For Neoplastic lesions one should do specific tumor markers and screening of whole body to rule out metastases elsewhere.
All Patients with spinal tuberculosis are started on antituberculosis treatment as Tuberculous spondylodiscitis is primary medical problem. Surgery reserved only for the patients with complications or potential complications (9). Only the patients who had lost neurological power to Frankel grade A,B,C,D or with sphincter involvement were advised surgery. 11 patients who did not show good response to ATT after 3 months were also operated. 17 patients who had progressive kyphosis and instability due to more than 2 vertebral level involvement were also advised surgery. Operative management gives satisfactory results in elderly patients with tuberculous spondylodiscitis (21). Single level involvement of spinal tuberculosis can be very well dealt by posterior approach only ( Transpedicular decompression, 2 level above and 2 level below fixation and shortening). The posterior approach provides adequate exposure for decompression and rigid fixation, providing satisfactory clinical and radiological outcomes (21).
2 level involvement requires pasterolateral extraplueral approach for decompression and reconstruction ( 3 or 4 level above and below ). In case of more than 2 levels are involved one should think of anterior or anterior and posterior approach for thorough decompression and stabilization of segment involved.
The pathological fractures due to neoplastic inlvolvement require a thorough check up to determine the general condition of the patient, staging and grading of the tumor, life expectancy , anticipated hospital and ICU stay etc. The indications for surgery for primary lesions are neurological deficit, instability, intratctable pain, radioresistant tumor and not sensitive to chemotherapy. The metastatic lesion may need surgery for severe pain, progressive neurogical deficit, instability affecting ambulatory ability or solitary metastases where in complete excision may be advocated.
The decision of surgery in malignant or metastatic lesion is taken only if the general condition allows the patient to recover without significant postoperative morbidity or ICU stay.
Vertebroplasty or kyphoplasty is the modality used in such inoperable painful collapse. Transpedicle body augmenter Vertebroplasty proved to be safe and effective in reducing pain andimproving functional status of patients with spinal tumor (18). Percutaneous Vertebroplasty (PVP) can be an effective treatment for metastatic spinal tumors in patients even with posterior wall deficiency (16).
Takayuki Yamashita stated that palliative surgery benefited half of the patients with metastatic spinal tumor, with a greater probability of benefit found in persons with a higher total revised Tokuhashi score (score 9–15) and/or primary cancers with longer survival times (19).
The modified Tokuhashi scoring system is used to decide the operability of the tumor.
The type of surgery and approach is decided depending upon primary or metastasis, extent of involvement of vertebra (Tomita classification) and expected morbidity of the surgery. The response of the tumor to radiotherapy and chemotherapy is also an important factor in management. David W. Polly et al concluded that there is a strong recommendation for posterior or posterolateral approach from T2 through T5. For the T6–L5 regions of the spine we recommend either anterior, posterior, or combined anterior and posterior surgery depending on the clinical presentation, surgeon and patient preference (20).
Hormonal treatment and immunotherapy may play an important role in certain tumors like Ca breast, ovary. In some inoperable tumors management to control pain is very important.
The pathological fractures in elderly can be managed by the following algorithms.
References
1. Cicala D, Briganti F, Casale L, et al. Atraumatic vertebral compression fractures: differential diagnosis between benignosteoporotic and malignant fractures by MRI. MusculoskeletSurg 2013;97(Suppl. 2):169–79.
2. Asdourian PL. Metastatic disease of the spine. In: Bridwell KH, DeWald RL, eds. The Textbook of Spinal Surgery. Philadelphia, JB Lippincott, 1991:1187-242. [Context Link]
3. Cybulski GR. Method of surgical stabilization for metastatic disease of the spine. Neurosurgery 1989;25:240-52. Buy Now Bibliographic Links [Context Link]
4. Hammerberg KW. Surgical treatment of metastatic spine disease. Spine 1992;17:1148-53. [Context Link]
5. Sundaresan N, Galicich JH, Lane JM. Harrington rod stabilization for pathological fractures of the spine. J Neurosurg 1984;60:282-6.Bibliographic Links [Context Link]
6. Matsubayashi T, Koga H, Nishiyama Y, et al. The reparative process of metastatic bone lesions after radiotherapy. Japan J ClinOncol 1981;11(Suppl):253. [Context Link]
7. Svanhild Waterloo, Luai A Ahmed et al. Prevalence of vertebral fractures in women and men in the population-based Tromsø Study. BMC Musculoskeletal Disorders 2012, 13:3
8. Naim-Ur-Rahman, El-Bakry A, Jamjoom A, et al. Atypical forms of spinal tuberculosis: case report and review of the literature. Surg Neurol. 1999;51(6):602- 07.
9. Rasouli MR, Mirkoohi M, Vaccaro AR, Yarandi KK, Rahimi-Movaghar V. Spinal Tuberculosis: Diagnosis and Management. Asian Spine J. 2012;6(4):294–308.
10. Jung NY, Jee WH, Ha KY, Park CK, Byun JY. Discrimination of tuberculous spondylitis from pyogenic spondylitis on MRI. AJR Am J Roentgenol. 2004;182(6):1405-10.
11. Khattry N, Thulkar S, Das A, Alan Khan S, Bakhshi S. Spinal tuberculosis mimicking malignancy: Atypical imaging features. Indian J Paediatr. 2007;74(3):297-8. PMID: 17401273.
12. Moore SL, Rafii M. Imaging of musculoskeletal and spinal tuberculosis. RadiolClin North Am. 2001;39(2):329-42.
13. Momjian R, George M. Atypical Imaging Features of Tuberculous Spondylitis: Case Report with Literature Review. J Radiol Case Rep. 2014;8(11):1–14.
14. Tan DY , Tsou IY , Chee TS. Differentiation of malignant vertebral collapse from osteoporotic and other benign causes using magnetic resonance imaging. Annals of the Academy of Medicine, Singapore [2002, 31(1):8-14]
15. Max Aebi. Spinal metastasis in the elderly .Eur Spine J (2003) 12 (Suppl. 2) : S202–S213
16. Hongpu Sun et al Safety of percutaneous vertebroplasty for the treatment of metastatic spinal tumors in patients with posterior wall defects. Eur Spine J (2015) 24:1768–1777
17. J. Tehranzadeh, C. Tao & C. A. Browning (2007) Percutaneous Needle Biopsy of the Spine, Acta Radiologica, 48:8, 860-868.
18. Anna F-Y. Li, Kung-Chia Li, Fang-Yuan Chang and Ching-Hsiang Hsieh. Preliminary Report of Transpedicle Body Augmenter Vertebroplasty in Painful Vertebral Tumors. SPINE Volume 31, Number 21, pp E805–E812 ©2006.
19. Takayuki Yamashita, Yoichi Aota et al Changes in Physical Function After Palliative Surgery for Metastatic Spinal Tumor Association of the Revised Tokuhashi Score With Neurologic Recovery. SPINE Volume 33, Number 21, pp 2341–2346 ©2008
20. David W. Polly, Jr, Dean Chou et al. An Analysis of Decision Making and Treatment in Thoracolumbar Metastases. SPINE Volume 34, Number 22S, pp S118–S127 ©2009.
21. Manish Kothari, Kunal Shah, Agnivesh Tikoo, Abhay Nene. Short to Mid-Term Term Surgical Outcome Study with Posterior Only Approach on Tuberculous Spondylodiscitis in an Elderly Population. Asian Spine J 2016;10(2):258-266.
| How to Cite this Article: Parasnis R, Thumbadiya A, Pathak S, Patil S. Management of Pathological vertebral collapse in elderly. International Journal of Spine Sep-Dec 2016;1(2):22-26. |

(Abstract) (Full Text HTML) (Download PDF)
Taking IJS Ahead
Volume 1 | Issue 2 | Sep – Dec 2016 | Page 1-2 | Ketan Khurjekar [1], Shailesh Hadgaonkar [1], Ashok Shyam [1,2]
Authors : Ketan Khurjekar [1], Shailesh Hadgaonkar [1], Ashok Shyam [1],[2]
[1] Sancheti Institute for Orthopaedics &Rehabilitation, Pune, India
[2] Indian Orthopaedic Research Group, Thane, India
Address of Correspondence
IJS Editorial Officie
A-203, Manthan Apts, Shreesh CHS, Hajuri Road, Thane [W]
Maharashtra, India.
Email: editor.ijspine@gmail.com
International Journal of Spine has made its mark from the release of first issue and in the second issue we have tried to make it better. As mentioned in the first editorial IJS has two main focus points, Research as well as Education. Currently most of the journals are focussed on research based articles and almost 90% of their publication is original articles. IJs is planned to take a different route where we wish to include equal amount of educational material in the journal.
Every issue of IJS is planned to contain a symposia on a specific topic. These symposia are solicited from leading spine surgeons in the field and are formatted in form of a review article which is easy to read. We encourage authors to include case based scenarios in the review which become much easier to relate to a clinician unlike articles full of statistics. The symposium are created in such a way that even small topics related to the scope of symposia are given adequate space and not become part of foot note. This approach will help general orthopaedic surgeons also who wish to refresh their knowledge and update themselves in the field of spine surgery. This will be especially useful to students who can get collection of articles on single topic written by best authors at one place. We will continue this trend of symposia in all future issue of IJS and invite suggestions from our readers for the topic of symposia. We also invite interested surgeons who wish to be symposium editors to contact the editorial office.
Short narrative reviews and literature updates also form the education element in IJS. One narrative review is published in this issue and from next issue the literature updates will start. It will include summary of most important articles and research that are published in other spine journals and are of practical importance to our readers. Original research articles and case reports will continue to be published in the journal but with strict review guidelines and will follow all ethical standards
From this issue we have started a new feature called ‘Interview’. IJS intends to interview the role models in field of spine surgery, especially people who inspire us to achieve excellence. The aim is to know them better and to understand their though process. We can learn many things from them even outside orthopaedics and this aspect comes out beautifully in the current interview of Dr S Rajasekaran. He was gracious enough to give us his precious time and share with us his knowledge and principles that he follows in his life. We believe this interview will inspire many and everyone will learn something valuable from it. The interview was almost two hours long and in this issue we could include only the part of the interview. The second part will be published in the forthcoming issue. We wish to continue this feature and will be interviewing many more stalwarts in the field of Spine surgery.
IJS is receiving more and more submissions each day and we wish to continue publishing good quality articles. We will appreciate any suggestions of comments, please write to us by email to editor.ijspine@gmail.com.
Dr. Ketan Khurjekar | Dr. Shailesh Hadgaonkar | Dr. Ashok Shyam
| How to Cite this Article: Khurjekar K, Hadgaonkar S, Shyam A. Taking IJS Ahead. International Journal of Spine Sep – Dec 2016;1(2):1-2. |

(Abstract) (Full Text HTML) (Download PDF)
Cervical Ossified Posterior Longitudinal Ligament
Volume 1 | Issue 2 | Sep – Dec 2016 | Page 49-51 | Kunal Shah, Manish Kothari, Abhay Nene
Authors : Kunal Shah [1], Manish Kothari [1], Abhay Nene [1]
[1] Department of Spine Surgery, Wockhardt Hospital and
Medical Research Centre Agripada, Dr Anand Rao Nair Road
Mumbai Central, Mumbai. India – 400008
Address of Correspondence
Dr. Abhay Nene
Department of Spine Surgery, Wockhardt Hospital and
Medical Research Centre Agripada, Dr Anand Rao Nair
Road,Mumbai Central, Mumbai. India – 400008
Email: abhaynene@yahoo.com
Abstract
Introduction
Cervical ossified posterior longitudinal
ligament is a common cause of myelopathy.
It is frequently encountered in busy spine
clinic with varied presentation; however
there are lots of controversies in this topic.
Etiopathogenesis and natural history is
unknown and progression is unpredictable.
Timing of surgery and type of approach is
also controversial and many factors should
be taken into account for surgical planning.
References
1) Yonenobu K. Is surgery indicated for asymptomatic or mildly
myelopathic patients with significant ossification of the posterior
longitudinal ligament? Spine (Phila Pa 1976). 2012 Mar
1;37(5):E315-7.
2) Wilson JR, Patel AA, Brodt ED, Dettori JR, Brodke DS, Fehlings MG.
Genetics and heritability of cervical spondylotic myelopathy and
ossification of the posterior longitudinal ligament: results of a
systematic review. Spine (Phila Pa 1976). 2013 Oct 15;38(22 Suppl
1):S123-46.
3) Chiba K , Yamamoto I , Hirabayashi H , et al. Multicenter study to
investigate postoperative progression of the posterior longitudinal
ligament in the cervical spine using a new computer-assisted
measurement . J Neurosurg Spine 2005 ; 3 : 17 – 23 .
4) Choi BW, Baek DH, Sheffler LC, Chang H. Analysis of progression of
cervical OPLL using computerized tomography: typical sign of
maturation of OPLL mass. J Neurosurg Spine. 2015 Jul 17:1-5.
5) Matsunaga S , Sakou T , Hayashi K , et al. Trauma-induced
myelopathy in patients with ossifi cation of the posterior longitudinal
ligament . J Neurosurg 2002 ; 97 : S172 – 5 .
6) Matsunaga S , Kukita M , Hayashi K , et al. Pathogenesis of
myelopathy in patients with ossifi cation of the posterior longitudinal
ligament . J Neurosurg 2002 ; 96 : S168 – 72 .
7) Matsunaga S, Nakamura K, Seichi A, Yokoyama T, Toh S, Ichimura S,
Satomi K, Endo K, Yamamoto K, Kato Y, Ito T, Tokuhashi Y, Uchida K,
Baba H, Kawahara N, Tomita K, Matsuyama Y, Ishiguro N, Iwasaki M,
Yoshikawa H, Yonenobu K, Kawakami M, Yoshida M, Inoue S, Tani T,
Kaneko K, Taguchi T, Imakiire T, Komiya S. Radiographic predictors
for the development of myelopathy in patients with ossification of the
posterior longitudinal ligament: a multicenter cohort study. Spine
(Phila Pa 1976). 2008 Nov 15;33(24):2648-50.
8) Rhee JM, Shamji MF, Erwin WM, Bransford RJ, Yoon ST, Smith JS,
Kim HJ, Ely CG, Dettori JR, Patel AA, Kalsi-Ryan S. Nonoperative
management of cervical myelopathy: a systematic review. Spine
(Phila Pa 1976). 2013 Oct 15;38(22 Suppl 1):S55-67.
9) Yoon ST, Raich A, Hashimoto RE, Riew KD, Shaffrey CI, Rhee JM,
Tetreault LA, Skelly AC, Fehlings MG. Predictive factors affecting
outcome after cervical laminoplasty. Spine (Phila Pa 1976). 2013 Oct
15;38(22 Suppl 1):S232-52.
10) Iwasaki M, Okuda S, Miyauchi A, Sakaura H, Mukai Y, Yonenobu K,
Yoshikawa H. Surgical strategy for cervical myelopathy due to
ossification of the posterior longitudinal ligament: Part 2: Advantages
of anterior decompression and fusion over laminoplasty. Spine (Phila
Pa 1976). 2007 Mar 15;32(6):654-60.
11) Suda K , Abumi K , Ito M , et al. Local kyphosis reduces outcomes of
expansive open-door laminoplasty for cervical spondylotic
myelopathy . Spine 2003 ; 28 : 1258 – 62 .
12) Sakai K, Okawa A, Takahashi M, Arai Y, Kawabata S, Enomoto M,
Kato T, Hirai T, Shinomiya K. Five-year follow-up evaluation of
surgical treatment for cervical myelopathy caused by ossification of
the posterior longitudinal ligament: a prospective comparative study
of anterior decompression and fusion with floating method versus
laminoplasty. Spine (Phila Pa 1976). 2012 Mar 1;37(5):367-76.
13) Katsumi K, Izumi T, Ito T, Hirano T, Watanabe K, Ohashi M. Posterior
instrumented fusion suppresses the progression of ossification of the
posterior longitudinal ligament: a comparison of laminoplasty with and
without instrumented fusion by three-dimensional analysis. Eur Spine
J. 2015 Nov 19. [Epub ahead of print]
14) Wei-bing X , Wun-Jer S , Gang L , et al. Reconstructive techniques
study after anterior decompression of multilevel cervical spondylotic
myelopathy . J Spinal Disord Tech 2009 ; 22 : 511 – 5 .
15) Yamaura I, Kurosa Y, Matuoka T, et al. Anterior floating method for
cervical myelopathy caused by ossification of the posterior
longitudinal ligament. Clin Orthop 1999;359:27–34.
| How to Cite this Article: Shah K , Kothari M , Nene A. Cervical Ossified Posterior Longitudinal Ligament. International Journal of Spine Sep-Dec 2016;1(2): 49-51. |
(Abstract) (Full Text HTML) (Download PDF)
An epidemiological study from a tertiary care hospital in Asian subcontinent on Traumatic cervical injuries: How is the injury pattern and what are the implications?
Volume 1 | Issue 2 | Sep – Dec 2016 | Page 44-48 | Dhiraj Vithal Sonawane, Ganesh Yeotiwad, Ajay Chandanwale, Swapnil Keny, Abhijeet Salunke, Ambarish Mathesul, Eknath Pawar
Authors : Dhiraj Vithal Sonawane [1], Ganesh Yeotiwad [1], Ajay Chandanwale [3], Swapnil Keny [1], Abhijeet Salunke [4], Ambarish Mathesul [3], Eknath Pawar [2]
[1] Department of Orthopaedics, Grant Medical college, & Gokuldas Tejpal Hospital, Mumbai
[2] Department Of Orthopaedics, Grant medical college, Mumbai.
[3] Sasoon Hospital & BJMC, Pune
[4] Gujarat Cancer Research Institute
Address of Correspondence
Dr. Dhiraj V. Sonawane
Grant Medical college, & Gokuldas
Tejpal Hospital, Mumbai
Email: dvsortho@gmail.com
Abstract
Objective: The aim of the current study was to document the demographic pattern, mode of injury, level of cervical spine injury in patients so that it can be extrapolated for formulating guidelines in developing nations for proper management of this life threatening injury.
Methods: This study comprised of 275 patients of cervical spine injury admitted in a tertiary care centre from January 2006 to October 2015.
Results: The mean age was (3 to 95) and male to female ratio was 11.5: 1. Majority (30 %) of cases were of third and fourth decade. 60 % of patient fall from height as mechanism of injury. The urban to rural ratio of patients was 3:1 and 184 patients (67%) belonged to the rural areas. The most common mode of injury in the present study was fall from height, 166 cases (60%) of which most of them occurred while working and fall from tree. Dislocation at C 5-6 vertebral level was commonest and a C 5 vertebra was most commonly fractured. Incomplete cord injury of ASIA grade C scale was the commonest pattern seen in 156 cases. Head injury was commonest associated injury with cervical spine injury.
Conclusion: Identification of demographic data and mechanism of injury pattern helps to identify the preventable risk factors for controlling them. Proper education and training of paramedical staff in rural areas of initial aid and transportation of patients having spinal cord injuries can reduce the frequency and morbidity of spine injuries
Keywords: Cervical spine, Injury, Epidemiology, demographic study, Spinal cord, Mechanism of injury
References
1. David O`Brien. Immediate management of spinal injury In: Jones D.
Palmar (compiler) manual of neurosurgery. First edition, UK,
Churchill, Livingston. 1996; 696-708
2. George W. Wood II, Campbell’s Operative Orthopaedics, 11th ed., vol
1, Elsevier, Philadelphia; 1761-1849.
3. Sinha DK. Manual of Patna Model for the care of Spinal cord injury
patients. Patna: Sparsh. 2000; 9-13.
4. Roopsingh et al. Traumatic spinal cord injuries in Haryana: An
Epidemiological study.Indian Journal of Community Medicine Vol.
XXVIII, No.4, Oct.-Dec., 2003.
5. Gunby I. New focus on spinal cord injury.JAMA.1981;245:1201–1206.
6. Botterell EH, Jousse AT, Kraus AS et al.A model for the future care of
acute spinal cord injuries.Can J NeurolSci. 1975; 2:361-80 .
7. Kraus JF. Injury to the head and spinal cord: The epidemiological
relevance of the medical literature published from 1960 to 1978.J
Neurosurg. 1980; S: S3-10.
8. Burney R.E. et al. Incidence ,Characteristicsand Outcome of Spinal
Cord Injury at Trauma Centers in North America .Arch Surg. 1993;
128 (5):p.596-9.
9. Fife D.andJ.Kraus .Anatomic Location of Spinal Cord Injury:
Relationship to the cause of injury. Spine. 1986; 11 (1):p.2-5.
10. Riggins R.S.and J.F.Kraus. The Risk of Neurologic Damage with
Fractures to the Vertebrae.The Journal of Trauma. 1977; 17 (2): p.
126-133.
11. Miller T.R.,et al. Costs of Head and Neck Injury and a Benefit –Cost.
12. Allen B.L. et al. A Mechanistic Classification of Closed,Indirect
Fractures and Dislocation of the Lower Cervical Spine. 1982;
7(1):p.1-27.
13. Burke D.C., H.T.Burleyand G.H.Ungar. Data on Spinal Injuries –Part
1.Collection and Analysis of 352 Consecutive Admissions
.AustrN.Z.Surg. 1985; 55:p.3-12.
14. Torg J.S., et al. National Football Head and Neck Injury Registry:
Report on Cervical Quadriplegia .AM J Sports Med. 1979;
7 (2):p.127-32.
15. Annamalai K, Chinnathambi R. Spinal cord injuires -The challenges
and the achievements. Chennai: Dept.of Orthopaedic Surgery,
Govt. General Hospital,Chennai.1998; 1-50.
16. Karacan I, Koyuncu H, Pekel O, Sumbuloglu G, KirnapM, Dursum
H et al. Traumatic spinal cord injuries inTurkey: a nationwide
epidemiological study. Spina Cord. 2000; 38(11): 697-701.
17. Hu R, Mustard CA, Burns C. Epidemiology of incident spinal
fracture in a complete population.Spine.1996; 21:492-499.
18. Chacko V, Joseph B, Mohanty SP, Jacob T. Management of spinal
cord injury in a general hospital in rural India. Paraplegia.1996; 24:
330-5.
19. A psychological study of spinal cord injured patients involved in the
Madras Paraplegia ProjectO Somasundaram, S Balakrishnan, O S
Ravindran, T K Shanmugasundaram.
20. Shingu H, Ikata T, Katoh S, Akatsu T. Spinal cord injuries in Japan:
A natiowide epidemiological survey in 1990. Paraplegia 1994;
32(1): 3-8.
21. Lan C, Lai JS, Chang KH, Kan YC, Lein In. Traumatic spinal cord
injuries in the rural region of Taiwan: an epidemiological study in
Hualien Country, 1986-1990. Paraplegia 1993; 31(6): 398-403.
22. Dave PK, Jayaswal A, Kotwal PP. Spinal cord injuries -A clinicoepidemiological
study. Ind J Orthop 2002; 28: 39- 45.
23. Singh M et al. Spine injuries in a tertiary health care hospital in
Jammu: A Clinico – Epidemiological Study. The Internet Journal of
Neurosurgery.
24. Shrestha D, Garg M, Singh GK, Singh MP, Sharma Uk.Cervical
spine injuries in a teaching hospital of eastern region of Nepal; A
clinic-epidemiological study. J Nepal med Assoc 2007; 46(167):
107-111.
25. Hadley MN, Zabramski JM, Browner CM, et al. Pediatric spinal
trauma:review of 122 cases of spinal cord and vertebral column
injuries. J Neurosurg.1988;68:18–24.
26. Carreon LY, Glassman SD, Campbell MJ. Pediatric spinefractures:
a review of 137 hospital admissions. J Spinal DisordTech.2004;
17:477–482.
27. Parisini P, Di Silvestre M, Greggi T. Treatment of spinal fractures in
children and adolescents: long-term results in 44patients. Spine.
2004; 27:1989–1994. Thesleff T, 28)Niskakangas T, Luoto TM,
Öhman J, Ronkainen A. Fatal cervical spine injuries: a Finnish
nationwide register-based epidemiologic study on data from 1987
to 2010. Spine J. 2015 Dec 7. pii: S1529-9430(15)01761-1.
29. Fredø HL, Rizvi SAM, Lied B, Rønning P, Helseth E. The
epidemiology of traumatic cervical spine fractures: a prospective
population study from Norway.Scandinavian Journal of Trauma,
Resuscitation and Emergency Medicine. 2012;20:85.
30. Hasler RM, Exadaktylos AK, Bouamra O, Benneker LM, Clancy M,
Sieber R, Zimmermann H, Lecky F. Epidemiology and predictors of
cervical spine injury in adult major trauma patients: a multicenter
cohort study. J Trauma Acute Care Surg. 2012 Apr;72(4):975-81.
31. Rahimi-Movaghar V, Sayyah M, K, Akbari H, Khorramirouz R,
Rasouli M, R, Moradi-Lakeh M, Shokraneh F, Vaccaro A, R,
Epidemiology of Traumatic Spinal Cord Injury in Developing
Countries: A Systematic Review. Neuroepidemiology 2013;41:65-
85
32. Sidong Yang, Wenyuan Ding, Dalong Yang, Tixin Gu, Feng Zhang,
Di Zhang, Yapeng Sun, Lei Ma, Yanli Song.Epidemiology and Risk
Factors of Cervical Spine Injury during Heating Season in the
Patients with Cervical Trauma: A Cross-Sectional Study PLoS One.
2013; 8(11): e78358.
| How to Cite this Article: Sonawane D V, Yeotiwad G, Chandanwale A, Keny S, Salunke A, Mathesul A, Pawar E.An epidemiological study from a tertiary care hospital in Asian subcontinent on Traumatic cervical injuries: How is the injury pattern and what are the implications?. International Journal of Spine Sep-Dec 2016; 1(2): 44-48. |

