
Thoracolumbar Fractures – “Changing Perspectives”.
Volume 1 | Issue 2 | Sep – Dec 2016 | Page 9-13 | Raghava D Mulukutla
Authors : Raghava D Mulukutla [1]
[1] Director & Chief of Spine Surgery
Udai Omni & Apollo Health city
Hyderabad
Address of Correspondence
Dr. Raghava D.Mulukutla
Director & Chief of Spine Surgery
Udai Omni & Apollo Health city
Hyderabad.
Email: rdmuluk@gmail.com
Abstract
Road traffic accidents are commonest cause of Thoracolumbar fractures which may or may not be associated with neurological injuries. Most of the classification are purely descriptive, but recently focus has shifted in developing more prognostic classifications. Diffirent management approaches are defined depending on the fracture type and the scenario is still remains a dynamic and evolving one. The current review aims to provide an overview of changing perspectives in this field
Keywords: Thorocolumbar fractures, management options.
Introduction
The thoracic spine which is fixed and the lumbar spine which is mobile predisposes this area for fractures and it is not surprising that this area which is a transitional zone accounts for nearly 58% of spinal injuries [1]. Pre existing Osteopenia or osteoporosis and other metabolic disorders can precipitate fractures in this area. However severe injuries with or without neurological deficit are mostly due to road traffic accidents, fall from heights or industrial injuries. Since the early part of 20th century various classifications have emerged and till date there is no thoracolumbar fracture classification system that is perfect and classification systems are still evolving. Various treatment options including non operative treatments, short segment fusions, and more recently minimally invasive surgical techniques are used by surgeons in managing these injuries. It is important not to overlook other serious associated injuries and if present should be addressed first before undertaking surgery of thoracolumbar spinal injuries. Neurological deficits are not uncommon with more serious thoracolumbar trauma and it is important to protect the spine during transport and emergency stabilization of the patient up until final treatment [2].
The Ever Evolving Classifications
Classification of thoracolumbar fractures is important to identify stable and unstable injuries and help strategize treatment and to study the results of such treatments across various centres. Ideally, classifications should be easily understandable in clinical settings, reproducible, simple and direct the treating surgeon to appropriate management protocols. Newer classifications systems continue to emerge and is it is true to mention that there is no universally acceptable classification of thoracolumbar fractures.
The initial classification systems started with descriptive terms3 and later biomechanical factors such as anatomical regions and mechanical forces acting on the spinal column were introduced. Boehler [4] was the first to classify thoracolumbar fractures and he described five categories.
1. Compression fractures
2. Flexion –distraction injuries
3. Extension fractures with injury to anterior and posterior long. Ligament.
4. Shear fractures and
5. Rotational injuries
Watson Jones [5] introduced the concept of instability and was one of the first few to recognize the importance of posterior longitudinal ligament in maintaining spinal stability. There were seven types in his classification of Thoraco lumbar injuries with three major patterns: viz. a. simple wedge fractures b. comminuted fractures and c. Fracture dislocations

Nicoll [6] described anatomical classification and felt that the major determinant of stability was the interspinous ligament.3 Holdsworth7 was the first to coin the term “Burst Fracture” and introduced the “column concept” dividing the spine into two major columns : anterior column comprising the vertebral body and disc and the posterior column comprising the facet joints and posterior ligamentous complex. He felt that if both columns are disrupted the fracture would then be unstable. Kelly and Whitesides8 working on the Holdsworth concept felt that all burst fractures are inherently unstable.
With the advent of CT scans and after a review of 412 patients Denis presented his 3 column concept which is widely accepted [9]. He postulated that ALL (anterior longitudinal ligament), anterior half of the vertebral body and disc form the anterior column; PLL (Posterior longitudinal ligament) posterior half of vertebral body and disc constitute the middle column and the remaining posterior elements comprising the posterior column. The middle column according to Denis is the key for the stability of thoracolumbar fractures. Anterior column transmits 30% body weight and posterior column about 20%. However Anterior and Middle columns both resist 70-80% of body weight in flexion and the middle and posterior column resist 60% of body weight in extension. In Compression Fractures there is an anterior column failure and Burst fractures are secondary to Anterior and Middle column failure .Seat belt injuries are due to flexion distraction forces with failure of middle and posterior columns . In fracture dislocation all the three columns fail. Many surgeons do not agree that all Burst fractures are unstable; which is contrary to Denis classification where if two columns are involved in a fracture, then that fracture must be unstable [3,10].
The Holdsworth and Denis classification systems are anatomical classifications systems and they do not take into account the mechanisms of injuries of thoracolumbar fractures. McAfee [11] described a classification system where both the mechanism of injury and morphology of the fracture were included and he made the important contribution of describing the failure of the middle column due to a. axial compression b. axial distraction and c. translation.

Ferguson and Allen [12] proposed a mechanistic classification system and the mechanisms described are a. flexion compression, b. axial compression c. flexion distraction d. hyperextension –compression e. hyperextension distraction f. rotation –shear.
The AO – Magerl [13] classification and subsequent modifications of this classification system is very comprehensive and divides these injuries into Type A: compression; Type B : distraction and Type C : rotation and /or shear. Type A injuries are mostly simple and stable and Type C being very unstable injuries.
McCormack and Gains[14] described a Load sharing classification to predict implant failure and the need for additional Anterior surgery.
The Spine Trauma study group described the Thoracolumbar Injury Severity Score (TLISS) and The Thoracolumbar Injury classification and severity system (TLICS). This study based their severity scores on the a. mechanism of injury, b. integrity of Posterior ligament complex and c. the Neurologic status [15,16]. They recommended non operative treatment for scores less than 3 and surgery for scores more than 5 with a score of 4 to be treated with our without surgery [17].
Investigations:
AP and Lateral Radiographs, CT scans, MRI are all routinely used in the work up for thoracolumbar injuries. Standing lateral Radiographs and dynamic X-rays have little role in the acute setting but when safe to do and not uncomfortable to the patient are useful to monitor vertebral collapse, progression of deformity if any and overall sagittal alignment of the spine.18 Whilst CT scans are useful in accurate classification of the thoracolumbar fractures, they are especially useful to rule out a chance fracture.18 MRI is invaluable to identify epidural haematoma, SCIWORA, injury to the disc and most importantly the posterior ligamentous injury. With increasing availability of scanning machines, and with improvements in image quality, acquisition time, and image reformatting there has been a dramatic change in the commonly used algorithms [19].
Management Strategies
The steroid controversy : In the 1990s use of Methylprednisolone in the treatment of acute spinal cord injury became a routine following publication of NASCIS II trials [20,21]. However, Hurlbert et al [22] from an evidence based approach reported that methylprednisolone cannot be recommended for routine use in SCI. They also concluded that prolonged administration for up to 48 hours may be harmful to the patient and suggested that methylprednisolone should be considered to have investigational (unproven) status only. Most surgeons today have abandoned the use of methylprednisolone in the management of acute spinal cord injury following thoracolumbar trauma.
Compression Fractures
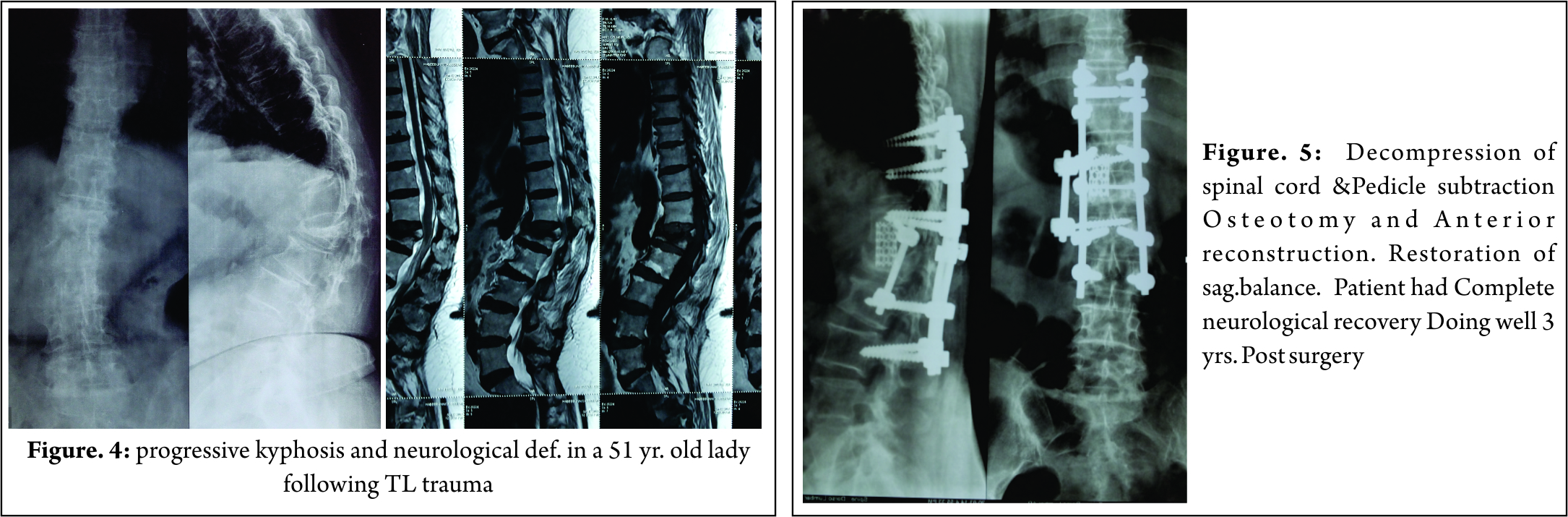
These injuries mostly involve the anterior column without involvement of the middle and posterior columns and are usually managed conservatively with analgesics, and restricted activity and strict bed rest may not be necessary. Most surgeons use front back support or TLSO or modifications of various hyper extension braces. However Giele et al [23] found no evidence to support that these braces are effective in Thoraco lumbar fractures. Vertebroplasty, Balloon Kyphoplasty are some of the procedures employed for pain relief. In those who present late with significant symptomatic kyphotic deformity or with late onset paraparesis, it is important to restore the sagittal balance with Pedicle subtraction osteotomy.
In spite of a large volume of literature on Burst fractures and their management, there is still no consensus on their management. The classification systems that are available are many and not universally acceptable leading further to the confusion about management of these injuries [24]. The problem is compounded when there is a neurological injury associated with these injuries. With fall from heights being the commonest cause of these injuries in India, the incidence of Neurological events is much higher at 60% compared to 40 % reported by various US studies [17].
Burst fractures are also classified as Stable and Unstable . Stable burst fractures are two column injuries. In the absence of neurological deficits and when not associated with other systemic injuries there is a trend amongst some surgeons to manage these injuries conservatively [25]. Those who manage these injuries conservatively believe that there is spontaneous remodeling of the spinal canal. However this view is not shared by many and conservative management demands regular radiological and clinical follow up to document late collapse and progression of kyphotic deformity.
Surgery: Neurological deficit and instability are definite indications for surgery in burst Thoraco lumbar fractures. In the presence of neurological deficit it is important to decompress the spinal cord. There is controversy regarding timing of surgery in those patients with neurological deficit. A few authors have advocated early surgery in patients with Neurological deficit [26], but there is no evidence that emergency surgical decompression has better outcomes. In the presence of progressive neurological deficit it is unwise to delay surgery and should be performed as early as possible. Controversy also exists as to the choice of approach in these fractures. McCormack based on their load sharing classification proposed that those with a score of 6 or less can be managed by posterior approach and those with a score of 7 or more should be managed by anterior approach. The anterior approach is indicated in those patients with extensive comminution of the vertebral body with severe retropulsion of fragments into the spinal canal. However there has been a recent trend to manage these burst fractures through a posterior only approach. Biomechanically placing short pedicle screws in the fractured vertebral body prevents implant failure. Short pedicle screws help in correcting the kyphotic deformity and in increasing the stiffness of the construct [2,27]. There is also controversy in literature about fusion following stabilization with some surgeons advocating fusion in predominantly ligamentous injuries [17].
Flexion –Distraction Injuries
Chance fractures or sea belt injuries are flexion distraction injuries with failure of all three columns in tension and the disruption of posterior elements may be osseous, ligamentous or both [28]. It is prudent to look for Intra abdominal injuries as they are sometimes associated with these injuries [29]. Some of these fractures without neurological deficit and in the absence of visceral injuries can be managed with a hyperextension brace. The trends in management of these fractures appears to be posterior approach when there is no neurological deficit or when there is a nerve root injury and in the presence of spinal cord or cauda equina injury a combined approach may be more appropriate [30].
Fracture Dislocations
According to TLICS classification these are inherently unstable injuries and need stabilization. They are typically 3 column injuries and it is commonly believed that pure hyperflexion or hyperextension alone may not produce thoracolumbar fracture dislocations and that there is always an additional rotational force that produces these injuries [31]. Fracture dislocations are associated with severe neurological deficits, except in those rare instances where a concomitant neural arch fracture may be associated with intact neurological function [32]
Biomechanics of Instrumentation
That Posterior pedicular instrumentation provides a slightly greater stiffness than anterior plate systems is proven by biomechanical studies. However these systems do not provide enough stiffness in axial rotation. Bence et al [33] believe that a combined approach is biomechanically superior to either an anterior or posterior approach alone in management of Thoraco lumbar trauma.
Long or Short constructs?
Opinion amongst surgeons is divided as to the number of levels to be instrumented in fractures of thoracolumbar spine. Short segment instrumentation has greater chance of instrumentation failure compared to longer constructs. However extending fusion to the lower lumbar vertebrae is not advisable and last instrumented vertebra should be L3 or above to minimise the risk of degeneration of lower lumbar discs [34].
The advantages of long segment constructs being that they resist bending forces much better than short segment instrumentation and help prevent kyphosis. There is also less pull out failure and a satisfactory spinal alignment can be achieved with long constructs [30]. According to Joseph et al [35]Short segment instrumentation is ideal for flexion distraction injuries.
Minimally Invasive Surgery In Thoraco Lubar Trauma(MIS)
MIS technologies are evolving and there is no long term studies to give definite guidelines. The posterior instrumentation by MIS technique works like an internal tension band while the fracture is healing. Some times anterior approaches are supplemented by MIS posterior instrumentation techniques.
Conclusions
Thoracolumbar trauma can range from simple fractures to more serious and complex fracture dislocations sometimes associated with life threatening injuries with or without neurological deficits. There is no universally acceptable classification system so far and some of these may not have much use in clinical settings. There are no randomized controlled trials comparing various treatment modalities and it is therefore not surprising that there is hardly any evidence based guidelines in the management of these injuries [30].
With better understanding of the morphology and mechanism of injury, a variety of treatment options are advocated for these injuries. There is a trend to manage stable burst fractures without neurological injury conservatively. However, more studies are needed to validate conservative treatment vs surgery, and in those with neurological deficits early vs. elective decompression of spinal cord and role of fusion in management of thoracolumbar fractures. It is important for the treating surgeon to understand the morphology of these fractures and the mechanisms responsible and plan and execute appropriate treatment strategies.
References
1.Leucht P, Fischer K, Muhr G et al. epidemiology of traumatic spine fractures. Injury 2009;40:166-72
2. Ajoy Shetty :Review Article,Thoraco lumbar Trauma :Journal of OASIS; 2011 p. 7-12
3.Uday M Pawar, Swapnil Keny, R.Chadda : Biomechanics and classification of Thoracolumbar Spinal Injuries:Ch. 44. ASSI Textbook of Spinal injuries and Trauma 2011;P.449-456
4.Boehler L. Die Techniek der Knochenbruchbehandlung im Grieden und im Kriegeed. Vienna , Austria: Verlag von Wilheim, Maudrich; 1930
5.Watson Jones R. The results of postural reduction of fractures of the spine. J Bone Joint surg Am. 1970;52:1534-51
6. Nicoll EA (1949) Fractures of the dorso-lumbar spine. J Bone Joint Surg Br 31:376–94
7. Holdsworth F (1970) Fractures, dislocations, and fracture-dislocations of the spine. J Bone Joint Surg Am 52:1534–51 56
8. Kelly RP, Whitesides TE (1968) Treatment of lumbodorsal fracture-dislocations. Ann Surg 167:705–17
9. Denis F (1983) The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine 8:817–31 31.
10. Agus H, Kayali C,Arslantas M. Non operative treatment of burst –type thoracolumbar vertebral fractures. Clinical and radiological results of 29 patients. Eur Spine J.2005;14:536-40
11. McAfee PC,Yuan HA,Friedrickson BE, et al. The value of computed Tomography in thoraco lumbar fractures. An analysis of one hundred consecutive cases and new classification. J Bone Joint Surg Am.1983;65: 461-73
12. Ferguson RL, Allen BL. A mechanistic classifiction of thoraco lumbar spine fractures. Clin Ortho Relat Res. 1984;(189):77-88
13. . Magerl F, Aebi M, Gertzbein SD, Harms J, Nazarian S (1994) A comprehensive classification of thoracic and lumbar injuries. Eur Spine J 3:184–201 81
14. McCormack T, Karaikovic E , Gains RW. The laod sharing classification of spine fractures .Spine (Phila Pa 1976)1994;19:1741-4
15. Sethi MK, Schoeffeld AJ, Bono CM et al. The evolution of thoraco lumbar injury classification systems. Spine J. 2009,9:780-8
16.Vaccaro AR,Zeiller SC,Hulbert RJ,et al : The thoraco lumbar injury severity score: a proposed tratment algorithm. J Spinal Disord Tech 2005;18:209
17.KV Menon, R Dalwai : Burst Fractures of Thoraco lumbar Spine : ASSI Text book of Spinal infections and Trauma :2011: Ch. 46; p462-470
18.A.Kulkarni, SM Shah :Vertebral compression Fractures, Ch. 45. ASSI Textbook of Spinal infections and Trauma 2011.P.457-461
19.Bagley LJ (2006) Imaging of spinal trauma. Radiol Clin North Am 44:1–12, vii
20.Bracken MB, Shepard MJ, Collins WF, et al: Methylprednisolone or naloxone treatment after acute spinal cord injury: 1-year follow-up data. Results of the second National Acute Spinal Cord Injury Study. J Neurosurg 76:23–31, 1992 5.
21.Bracken MB, Shepard MJ, Holford TR, et al: Administration of methylprednisolone for 24 or 48 hours or tirilazad mesylate for 48 hours in the treatment of acute spinal cord injury. Results of the third National Acute Spinal Cord Injury Randomized Controlled Trial. National Acute Spinal Cord Injury Study. JAMA 277:1597–1604, 1997
22.Hurlbert, R. John, The Role of Methylprednisolone in Acute Spinal Cord Injury
Spine: 2001 Issue 24S:- Vol 26 – pp S39-S46
23.Giele BM, Wiertsema SH, Beelen A et al. No evidence for effectiveness of bracing in patients wioth thoraco lumbar fractures. Acta Orthop. 2009;80:226-32
24Mirza SK, Mirza AJ, Chapman JR et al.Classification of thoraco lumbar fractures and their effect on treatment. J Am Acad Orthop Surg. 2002;10: 364-77
25.S.Rajasekharan. Thoraco lumbar fractures without neurological deficit: the role for conservative treatment. Eur Spine J.2010; 19(suppl 1):S40-S47
26.Krengel WF, Anderson PA, Henley MB. Early stabilisation and decompression for incomplete paraplegia due to thoracic level spinal cord injury. Spine. 1993; 18:2080-7
27.Mahar A,Kim C, Wedemeyer M, Mitsunaga L, Odell T, Johnson B, Graffin S. Short segment fixation of lumbar burst fractures using pedicle fixation at the level of fracture. Spine 2007Jun 15;32(14):1503-7
28.Groves CJ, Cassar-Pullicino VN,Tins BJ et al. Chance type flexion –distraction injuries in the throaco lumbar spine: MR imaging characteristics.Radiology.2005;236: 601 -8.
29.Chapman JR, Agel J, Jurkowich GJ,et al. Thoraco lumbar felxion –distraction injuries: associated morbidity and neurological outcomes.Spine (Phila Pa1976)2008;33:68-57
30.Harsh Priyadarshi,Thomas J kishen, Greg Etherington,Ashish D Diwan : Flexion –Distraction injuries and Fracture dislocations of the Thoracic and Lumbar spine. ASSI Text book of Spinal infections and Trauma :2011: Ch. 47; p 471-480
31.Roaf R. A study of the Mechanics of spinal injuries. J Bone Joint Surgery (Br). 1960;42-B (4):810-23
32.Gitelman A, Most MJ Stephen M. Traumatic thoracic spondyloptosis without neurological deficit and treatment with in situ fusion. Am J Orthop (Belle Mead NJ).2009;38:E 162-5
33.Bence T, Schreiber U Grupp T et al. Two column lesions in the Thoraco lumbar junction. Anterior, posterior or combined approach? A comparative biomechanical in vitro investigation. Eur J spine 2007;16:813-20
34.Mc Lain RF. The biomechanics of long versus short fixation for Thoraco lumbar spine fractures. Spine (Phila Pa 1976)2006;31:S 70-79ldiscussion s 104
35.Joseph Sa, Stephen M , Meinhard BP. The successful short term treatment of flexion distraction injuries of thoracic spine using posterior-only pedicle screw instrumentation. J spinal diso Tech. 2008;21:192-8.
| How to Cite this Article: Mulukutla RD. Thoracolumbar fractures – “Changing Perspectives”. International Journal of Spine Sep-Dec 2016;1(2):9-13. |


