
Osteoid Osteomas of Spine: From open to minimally invasive excision of the Nidus – A Case series
Volume 8 | Issue 1 | January-June 2023 | Page: 18-22 | S. Ganesh Kumar, Sudeep Kumar V.N, Sivakumar Raju, Vinoth Thangamani, Bharatkumar Ramalingam Jeyashankaran, Chidambaram Muthu
DOI: https://doi.org/10.13107/ijs.2023.v08.i01.47
Submitted: 10/01/2023; Reviewed: 23/01/2023; Accepted: 14/04/2023; Published: 10/06/2023
Authors: S. Ganesh Kumar [1], Sudeep Kumar V.N [1], Sivakumar Raju [1], Vinoth Thangamani [1], Bharatkumar Ramalingam Jeyashankaran [1], Chidambaram Muthu [1]
[1] Department of Spine Surgery, Preethi Hospitals, Melur Main Road, Uthangudi, Madurai, Tamil Nadu, India.
Address of Correspondence
Dr. S. Ganesh Kumar,
Post-Doctoral Fellow in Spine Surgery, Preethi Hospitals, Melur Main Road, Uthangudi, Madurai, Tamil Nadu, India.
E-mail: sgk.ortho@gmail.com
Abstract
Osteoid osteomas of spine are not uncommon and majority of which occurs in posterior elements of lumbar spine. Management of such lesions in spine ranges from open en bloc excision to percutaneous radiofrequency ablation. In this series, we have managed three cases of osteoid osteomas of spine, each managed differently from conventional open technique to minimally invasive method. All three cases underwent appropriate radiological investigations and followed by surgical excision of the lesion and histopathological analysis post-operatively. First case was managed with open excision of the lesion with conventional unilateral pedicle screw stabilisation. Second case, who underwent open excision of the lesion developed recurrence which was managed by re-excision without any further complications. Last case underwent microendoscopic quadrant tubular excision of the tumour with unilateral MISS with pedicle screws.
The technique of Microendoscopic quadrant tubular excision of posterior element benign tumour had advantages of small skin incision, less bleeding, clear macroscopic visualisation of the small tumour (enables complete excision of the nidus thus decreasing the recurrence), early mobilisation and shorter hospitalization with effective and complete excision of the tumour better than open method. Further, histological evidence of tumour will be available. The complete excision of nidus using microendoscopic tubular retractors with unilateral fixation in young age gives encouraging results. This case series is followed by review of literature highlighting the role of COX-2 inhibitors in osteoid osteoma, cause for scoliosis and neurological deficit in osteoid osteoma and management of osteoid osteomas of spine.
Keywords: Tumor, Osteoid osteoma, Minimally invasive, Dorsolumbar spine, Excision biopsy
Introduction:
Osteoid osteoma is a benign and solitary bone forming tumour, making 10% of benign tumours of bone [1]. 10% – 25% occurs in spine, with preponderance (70%-100%) to posterior elements of spine, for unknown reasons [1,2,3]. Of these, about 56% occurs in lumbar spine [4]. Treatment for osteoid osteoma aims at complete removal of the nidus to prevent recurrences. Recently, minimally invasive techniques have been commonly used for the treatment degenerative spine diseases. In this series, we report three cases of osteoid osteoma of spine, one of which is managed through minimally invasive technique using microendoscopic quadrant tubular retractors.
Materials and Methods:
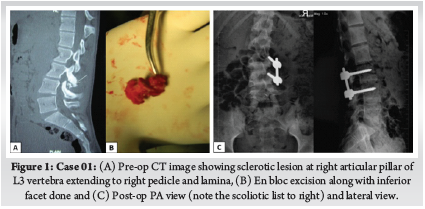
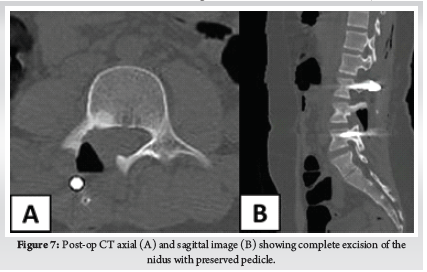
Our first case is a 15-year-old-boy, who had lower back pain (LBP) for 8 months with neither radicuolpathy nor signs of nerve irritation. Pain relieved by non-steroidal anti-inflammatory drugs (NSAIDS). Computed Tomography (CT) revealed a sclerotic lesion at right articular pillar of L3 vertebra extending to right pedicle and lamina with scoliotic list to right (Fig.1). He underwent open en bloc excision of the lesion and unilateral stabilisation with pedicle screws on L3-L4.
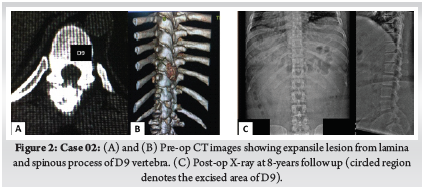
Second case, 36-year-old-male with pain in mid back region for 1 year duration, which has increased for last 15 days and not relieved by NSAIDS and also interfering with activities of his daily living. There was no symptoms or signs of nerve irritation. CT revealed a expansile lesion from lamina and spinous process of D9 vertebra with epidural soft tissue mass and new bone formation (Fig.2). He underwent open en bloc excision of the spinous process and right lamina. One year later, he developed recurrence, which was reoperated with wide local excision of the lesion. At 8-years follow up, no further recurrences noted.
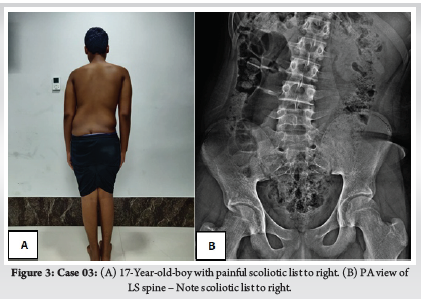
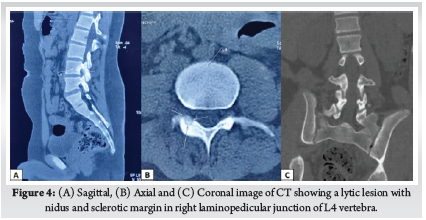
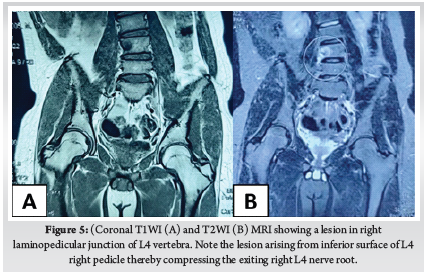
Third case is a 17-year-old-boy with LBP for 6 months of duration. At 2nd month of his symptom, he has undergone Magnetic Resonance Imaging (MRI), which was reported as normal study. He presented at 6th month of his symptom to our out-patient department (OPD) with persistent low back pain not relieved with NSAIDS and right lower limb radiculopathy with scoliotic list towards right (Fig. 3A). On examination there was weakness of right tibialis anterior with diminished sensation over right L4 dermatome. X-ray was taken which showed no obvious abnormality other than scoliotic list towards right (Fig. 3B). CT (Fig. 4) and MRI (Fig. 5) revealed a lytic lesion with nidus and sclerotic margin in right laminopedicular junction of L4 vertebra. Pre-operative Visual Analog Scale (VAS) for LBP was obtained. Excisional biopsy of the nidus with microendoscopic quadrant tubular retractors was performed. The details of all three cases are depicted in Table 1.
Surgical Technique:
The first and second case were operated through conventional open en bloc excision with addition of unilateral pedicle screw stabilisation for the former.
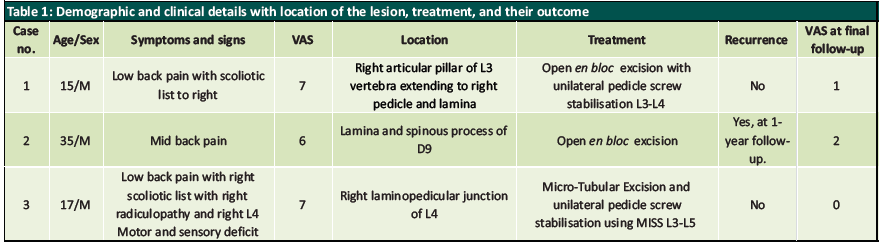
Third patient underwent excision of the nidus using microendoscopic quadrant tubular retractors. After positioning the patient in prone under general anaesthesia, fluoroscopy was performed intraoperatively before skin incision to know the exact location of insertion of quadrant tubular retractors. A 2cm skin incision was made 1.5 cm lateral to spinous process of L4 and after dorso-lumbar fasciotomy, the first dilator was docked at right spinolaminar junction of L4 vertebra. Then serial dilators (Medtronic Quadrant Tubular System) were inserted. Final dilator of size 22mm with 5mm depth was inserted and mounted to flexible arm attached to operating table (Fig. 6A). Right hemilaminectomy of L4 vertebra with facetal sparing was done. Then the nidus was reconfirmed under fluoroscopy and using microscope and burr, complete en bloc excision of nidus was done. The surrounding reactive tissues were also removed using rongeurs and curettes. After excision of the nidus, the exiting right L4 nerve root was found to be inflamed and oedematous (Fig. 6B). Then unilateral Minimally Invasive Surgical Stabilisation (MISS) with pedicle screws was done on ipsilateral pedicles of L3 and L5 vertebra (Fig. 6C). After haemostasis, wound closed with 3-0 ethilon. The patient was called for follow-up visits at regular intervals. Post-op VAS score was recorded. No complications were reported intra-operatively in all three cases. Histopathological Examination (HPE) of nidus of all three cases was done and were diagnostic of osteoid osteoma.
Results:
First case, recovered completely without any complications nor recurrence till 2-year follow-up. We have recommended implant removal after skeletal maturity, but for unknown reasons the patient lost his follow-up. Second case developed recurrence one year later and was reoperated with complete en bloc excision. No recurrences till 8-year follow-up with occasional pain only on intense activity.
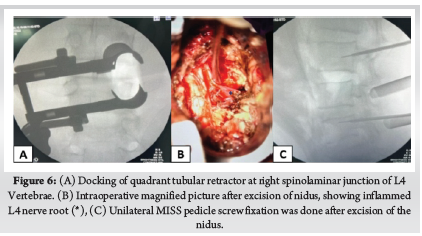
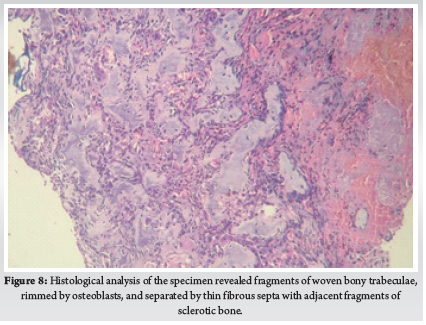
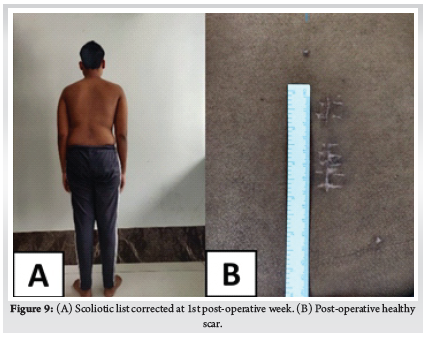
For the third case, the operative time was 90 minutes without significant blood loss. The radicular pain disappeared at once after surgery. The VAS score improved from 7/10 to 2/10 at immediate post-op period. The patient was made to walk on the evening of surgery and discharged on second post-operative day. Post-op CT showed the complete excision of the nidus with most of the pedicle kept intact (Fig. 7). HPE of the specimen (Fig. 8) confirmed our diagnosis. The scoliotic list resolved at first week (Fig. 9). The resolution of L4 neurological deficit occurred at sixth week. At second year follow-up visit, patient recovered completely without any complications nor recurrence.
Discussion:
Osteoid osteoma of spine is not an uncommon cause of LBP in adolescents presenting to ortho OPD. It is easily missed on first radiography due to its smaller size and complex anatomy of spine [5]. This is further complicated by highly variable appearance on MRI leading to its missed diagnosis [6]. This might be the reason our third case was initially missed, despite taking MRI initially. MRI may not clearly visualise the nidus and may only show peri-nidal marrow edema which might be confused with infection. CT scan is the most specific imaging modality in diagnosis of nidus [7]. A high level of cyclooxygenase-2 (COX-2) expression in neoplastic osteoblasts in the nidus of osteoid osteomas may cause the secondary changes depicted by MRI [8] and COX-2 is one of the important mediators of this condition [9] and this is the principle behind the use of NSAIDS in these lesions.
Almost two-third of osteoid osteoma of spine presents with painful scoliosis clinically [10]. Scoliosis in these patients is due to paravertebral muscle spasm and initially will be a non-structural one [11] later developing to a structural curve. A study by Ransford et al [12], reported that scoliosis persisted in patients who were operated after 15 months of symptoms. Delay in treatment might lead to persistence of scoliosis and becoming a structural one. So, the timing of treatment in those presenting with painful scoliosis is invaluable. In our series, two cases had scoliotic list, and both recovered after the excision of nidus. In both cases, the nidus was seen at concave side of the curve.
So far, no case of neurological deficit has been reported in the literature due to spinal osteoid osteoma [13]. Though spinal osteoid osteoma occurs close to neurological structures, deficit rarely occurs due to its small size [14]. Radiculopathy has been reported due to reactive inflammation caused by tumour [15]. In our series, first and second case had no symptoms or signs of nerve irritation. But third patient had right radiculopathy typically radiating along anterolateral aspect of thigh and medial aspect of leg with weakness of right ankle dorsiflexion and diminished sensation over medial malleolus. The neurological deficit in our case was due to reactive tissue arising from the inferior surface of L4 pedicle, which was compressing the right L4 nerve root as seen in pre-operative MRI (Fig. 5) .
The management of osteoid osteoma aims at complete excision or deactivation of the nidus to prevent the recurrences. Surgical excision is considered the optimal treatment modality for treating spinal osteoid osteoma [16]. The first and second case in our series was managed with open excision. One year after first surgery, second patient complained of pain at the same site, and was diagnosed with reactivation of lesion. Re-excision of the lesion was done and since the tumour was found at dorsal vertebra (D9), fixation was not done considering the inherent stability of dorsal vertebrae. The recurrence in this patient was due to incomplete excision of the lesion, which we think is a disadvantage of open excision due to difficulty in identifying the exact location of the lesion.
Radiofrequency ablation (RFA) is ideal choice if the nidus is located away from vital structures such as spinal cord, nerve roots and arteries. Rosenthal et. al [17, 18] who were the early pioneers of this method, suggested that the thermal necrosis was less safe if neural tissues were within 13 mm of the probe. Further, thin cortical bone of spine is not a reliable heat insulator and so percutaneous RFA for osteoid osteomas of spine carries a risk of neural damage [19]. Another disadvantage is histological evidence of osteoid osteoma is impossible with RFA. In our third case, the nidus was in such a location, where surgical excision would cause gross instability and RFA will be inappropriate as it is close to the right L4 nerve root. So, the microendoscopic quadrant tubular excision of the nidus was done with unilateral MISS pedicle screws on the same side pedicles of L3 and L5. This technique enables the magnified image of the nidus and its surrounding structures, which decreases the unnecessary wide bone resection, inadvertent injury to nerve roots and incomplete excision of the nidus as happened with our second case which resulted in recurrence of the tumour at 1-year.
Since, osteoid osteomas of spine are most common at pars interarticularis, its excision might cause instability which needs posterior stabilisation. In our series, 2 of 3 cases had nidus at pars interarticularis region. We did unilateral pedicle screw fixation using conventional open technique in first case and using MISS technique in third case. Unilateral pedicle screw fixation has advantages of decrease in operative time, length of hospital stays and blood loss with similar biomechanical advantage to bilateral pedicle screw fixation [20, 21]. Recently, Yang et al. [22] through their biomechanical study using finite element model and calf lumbar model, concluded that unilateral pedicle screw fixation is considered a safe and reliable technique. However, unilateral pedicle screw fixation has a disadvantage of increased cage migration, which is not applicable to our cases.
In open excision, the large surgical incision and inexact location of the nidus leads to incomplete excision of the nidus, increased paraspinal muscle damage with increased blood loss and creates bone defects which may require bone grafting, increasing the discomfort and expense of the patient [23, 24]. A case report of microendoscopic excision of C2 osteoid osteoma showed the advantages of minimal morbidity, minimal postoperative pain with less analgesic dependence, and better cosmesis [25]. The technique of microendoscopic quadrant tubular excision of posterior element benign tumour had advantages of small skin incision, less bleeding, clear macroscopic visualisation of the small tumour (enables complete excision of the nidus thus decreasing the recurrence), early mobilisation and shorter hospitalization with effective and complete excision of the tumour better than open method. Further, histological evidence of tumour will be available. With the advent of minimally invasive techniques, lesions of posterior element of spine can be safely excised and has more advantages than conventional open techniques.
Conclusion:
Osteoid osteomas of spine are easily missed due to their benign nature and variable appearance in imaging. So, high index of suspicion is needed in adolescent patients with painful scoliosis. The microendoscopic techniques using quadrant tubular retractor is already widely used for degenerative spinal diseases such as disc herniation, stenosis and facet cysts, its extended indication, as reported in our series, represents the newest and perhaps the most promising treatment for complete resection of tumours of this type. Thus, complete excision of nidus using microendoscopic tubular retractors with unilateral fixation in young age gives encouraging results.
References
[1] Gasbarrini, A., Cappuccio, M., Bandiera, S., Amendola, L., van Urk, P., & Boriani, S. (2011). Osteoid osteoma of the mobile spine: Surgical outcomes in 81 patients. Spine, 36(24), 2089–2093. https://doi.org/10.1097/BRS.0b013e3181ffeb5e
[2] Greenspan, A. (2004). Orthopedic Imaging: A Practical Approach. Lippincott Williams & Wilkins.
[3] Jackson, R. P., Reckling, F. W., & Mants, F. A. (1977). Osteoid osteoma and osteoblastoma. Similar histologic lesions with different natural histories. Clinical Orthopaedics and Related Research, 128, 303–313.
[4] Raskas, D. S., Graziano, G. P., Herzenberg, J. E., Heidelberger, K. P., & Hensinger, R. N. (1992). Osteoid osteoma and osteoblastoma of the spine. Journal of Spinal Disorders, 5(2), 204–211. https://doi.org/10.1097/00002517-199206000-00010
[5] Gamba, J., Martinez, S., Apple, J., Harrelson, J., & Nunley, J. (1984). Computed tomography of axial skeletal osteoid osteomas. American Journal of Roentgenology, 142(4), 769–772. https://doi.org/10.2214/ajr.142.4.769
[6] Davies, M., Cassar-Pullicino, V. N., Davies, A. M., McCall, I. W., & Tyrrell, P. N. M. (2002). The diagnostic accuracy of MR imaging in osteoid osteoma. Skeletal Radiology, 31(10), 559–569. https://doi.org/10.1007/s00256-002-0546-4
[7] Hosalkar, H. S., Garg, S., Moroz, L., Pollack, A., & Dormans, J. P. (2005). The diagnostic accuracy of MRI versus CT imaging for osteoid osteoma in children. Clinical Orthopaedics and Related Research, 433, 171–177. https://doi.org/10.1097/01.blo.0000151426.55933.be
[8] Kawaguchi, Y., Hasegawa, T., Oka, S., Sato, C., Arima, N., & Norimatsu, H. (2001). Mechanism of intramedullary high intensity area on T2-weighted magnetic resonance imaging in osteoid osteoma: A possible role of COX-2 expression. Pathology International, 51(12), 933–937. https://doi.org/10.1046/j.1440-1827.2001.01305.x
[9] Mungo, D. V., Zhang, X., O’Keefe, R. J., Rosier, R. N., Puzas, J. E., & Schwarz, E. M. (2002). COX-1 and COX-2 expression in osteoid osteomas. Journal of Orthopaedic Research: Official Publication of the Orthopaedic Research Society, 20(1), 159–162. https://doi.org/10.1016/S0736-0266(01)00065-1
[10] Janin, Y., Epstein, J. A., Carras, R., & Khan, A. (1981). Osteoid osteomas and osteoblastomas of the spine. Neurosurgery, 8(1), 31–38. https://doi.org/10.1227/00006123-198101000-00007
[11] Keim, H. A., & Reina, E. G. (1975). Osteoid-osteoma as a cause of scoliosis. The Journal of Bone and Joint Surgery. American Volume, 57(2), 159–163.
[12] Ransford, A. O., Pozo, J. L., Hutton, P. A., & Kirwan, E. O. (1984). The behaviour pattern of the scoliosis associated with osteoid osteoma or osteoblastoma of the spine. The Journal of Bone and Joint Surgery. British Volume, 66(1), 16–20. https://doi.org/10.1302/0301-620X.66B1.6693471
[13] Gasbarrini, A., Cappuccio, M., Bandiera, S., Amendola, L., van Urk, P., & Boriani, S. (2011). Osteoid osteoma of the mobile spine: Surgical outcomes in 81 patients. Spine, 36(24), 2089–2093. https://doi.org/10.1097/BRS.0b013e3181ffeb5e
[14] Zenmyo, M., Yamamoto, T., Ishidou, Y., Komiya, S., & Ijiri, K. (2011). Osteoid osteoma near the intervertebral foramen may induce radiculopathy through tumorous inflammation. Diagnostic Pathology, 6, 10. https://doi.org/10.1186/1746-1596-6-10
[15] Tekaya, A. B., Moalla, M., Salah, M. B., Saidane, O., Tekaya, R., Hadhri, K., Mahmoud, I., & Adbelmoula, L. (2021). Spinal Osteoid Osteoma Revealed by Radiculopathy: Case Report and Literature Review. International Journal of Spine Surgery, 14(s4), S26–S32. https://doi.org/10.14444/7161
[16] Mallepally, A. R., Mahajan, R., Pacha, S., Rustagi, T., Marathe, N., & Chhabra, H. S. (2020). Spinal osteoid osteoma: Surgical resection and review of literature. Surgical Neurology International, 11, 308. https://doi.org/10.25259/SNI_510_2020
[17] Rosenthal, D. I., Hornicek, F. J., Torriani, M., Gebhardt, M. C., & Mankin, H. J. (2003). Osteoid osteoma: Percutaneous treatment with radiofrequency energy. Radiology, 229(1), 171–175. https://doi.org/10.1148/radiol.2291021053
[18] Rosenthal, D. I., Springfield, D. S., Gebhardt, M. C., Rosenberg, A. E., & Mankin, H. J. (1995). Osteoid osteoma: Percutaneous radio-frequency ablation. Radiology, 197(2), 451–454. https://doi.org/10.1148/radiology.197.2.7480692
[19] Rybak, L. D., Gangi, A., Buy, X., La Rocca Vieira, R., & Wittig, J. (2010). Thermal ablation of spinal osteoid osteomas close to neural elements: Technical considerations. AJR. American Journal of Roentgenology, 195(4), W293-298. https://doi.org/10.2214/AJR.10.4192
[20] Lychagin, A., Cherepanov, V., Lipina, M., & Vyazankin, I. (2021). Comparison of the Unilateral and the Bilateral Pedicle Screw Fixation without Using an Interbody Cage: Randomized Clinical Trial. Open Access Macedonian Journal of Medical Sciences, 9(B), 398–402. https://doi.org/10.3889/oamjms.2021.6151
[21] Zhao, Y., Yang, S., & Ding, W. (2019). Unilateral versus bilateral pedicle screw fixation in lumbar fusion: A systematic review of overlapping meta-analyses. PloS One, 14(12), e0226848. https://doi.org/10.1371/journal.pone.0226848
[22] Yang, S., Xia, H., Cong, M., Guo, A., Ma, K., & Song, M. (2022). Unilateral pedicle screw fixation of lumber spine: A safe internal fixation method. Heliyon, 8, e11621. https://doi.org/10.1016/j.heliyon.2022.e11621
[23] Boscainos, P. J., Cousins, G. R., Kulshreshtha, R., Oliver, T. B., & Papagelopoulos, P. J. (2013). Osteoid osteoma. Orthopedics, 36(10), 792–800. https://doi.org/10.3928/01477447-20130920-10
[24] Çakar, M., Esenyel, C. Z., Seyran, M., Tekin, A. Ç., Adaş, M., Bayraktar, M. K., & Coşkun, Ü. (2015). Osteoid Osteoma Treated with Radiofrequency Ablation. Advances in Orthopedics, 2015, 807274. https://doi.org/10.1155/2015/807274
[25] Kulkarni, A. G., Dhruv, A. N., & Bassi, A. J. (2013). Microendoscopic excision of C2 osteoid osteoma: A technical report. Spine, 38(19), E1231-1234. https://doi.org/10.1097/BRS.0b013e31829cbf5e
| How to Cite this Article: Kumar SG, Sudeep Kumar VN, Raju S, Thangamani V, Jeyashankaran BR, Muthu C | Osteoid Osteomas of Spine: From Open to Minimally Invasive Excision of the Nidus – A Case series International Journal | of Spine | January-June 2023; 8(1): 18-22. |
(Full Text HTML) (Full Text PDF)
Surgical Management of Cervical Myelopathy: Current Algorithm
Volume 8 | Issue 1 | January-June 2023 | Page: 11-17 | Charanjit Singh Dhillon, Nilay Chhasatia
DOI: https://doi.org/10.13107/ijs.2023.v08.i01.46
Submitted: 13/02/2023; Reviewed: 10/04/2023; Accepted: 18/05/2023; Published: 10/06/2023
Authors: Charanjit Singh Dhillon [1], Nilay Chhasatia [1]
[1] Department of Spine Surgery, MIOT International, Chennai, Tamil Nadu, India.
Address of Correspondence
Dr. C. S. Dhillon,
Director-Spine Surgery, MIOT International, Chennai, Tamil Nadu, India.
E-mail: drdhillonc@hotmail.com
Abstract
Cervical myelopathy (CM) is a progressive disorder associated with a varied spectrum of etiological factors. Cervical spondylotic myelopathy (CSM) encompasses two-thirds of the cases of CM, while ossified posterior longitudinal ligament (OPLL) and ossified ligamentum flavum (OLF) are significant regional etiological factors. Microvascular disruption, resulting from repetitive dynamic compression or static pressure to the spinal cord, is attributed as a primary pathophysiological mechanism for CM. Magnetic resonance imaging (MRI) is the investigation of choice to assess the spinal cord. Lateral cervical radiographs are crucial for lordosis assessment, and tomographic scans (CT) can delineate the extent of OPLL and OLF. Non-surgical treatment is usually not successful once the patient develops progressive myelopathy. Anterior cervical procedures are ideal for one or two level disc-osteophytes complexes or in patients with kyphotic cervical alignment. Laminoplasty is an effective motion-preserving option in patients with adequate cervical lordosis. Laminectomy or laminoplasty and fusion are optimal for patients with significant preoperative neck pain. Posterior surgery is preferred over anterior surgery for CM involving three or more levels. Older age at presentation, longer duration of symptoms, and severity of pre-operative symptoms are adverse prognostic factors. Progressive cervical myelopathy is a surgical disease, and early intervention is rewarded with better outcomes.
Keywords: Cervical myelopathy, Cervical spondylotic myelopathy, OPLL, OLF, Laminoplasty, Laminectomy, ACDF, Cervical corpectomy.
INTRODUCTION AND ETIOLOGY
Cervical myelopathy (CM) encompasses a spectrum of disorders of varied etiology resulting in chronic and progressive compression of the spinal cord. Annual incidence has been predicted to be between 1.6-5.7 per 100,000 population in various series [1]. It is a disease of aging and most commonly seen in the 6th and 7th decade of life with a male preponderance. Degeneration of the cervical spine or cervical spondylosis (CS) is the most common cause of CM. Cervical spondylotic myelopathy (CSM) most commonly affects C4-5 and C5-6 levels, followed by C3-4 and C6-7 levels [1, 2]. The thickened ligamentum flavum, in conjunction with facetal hypertrophy, and osteophyte formation is responsible for around 60% of cases of degenerative CSM. Degenerative cervical spondylolisthesis is often associated with progressive myelopathy [3].
Degeneration in the dorsal and lumbar spine is also associated with the development of CSM. Thoracolumbar spinal deformity patients are twice as likely to present with myelopathic changes in the cervical spine compared to the healthy population. Arthritis in other joints such as hips and the temporomandibular joint is also reported to be associated with the onset of CSM [3].
Environmental factors also play a major role in the evolution of CSM. Certain professions or activities involving repeated jerky and vibratory motions significantly predispose an individual to the CSM. Drivers, weight lifters, drillers, and contact sportsmen such as ice-hockey players have a very high incidence of lifetime chronic neck pain and are predisposed to have early CSM [4]. This could be one of the reasons for a relatively higher preponderance of male patients to have symptomatic CSM.
In specific geographic loci, such as western and southern parts of India, ossified posterior longitudinal ligament (OPLL) and, to a lesser extent, ossified ligamentum flavum (OLF) contribute significantly to the prevalence of CM [5]. Both the static and dynamic biomechanical factors are implicated in the progression of myelopathic features due to the ossified ligaments. Progression of asymptomatic MRI positive OPLL patients to symptomatic myelopathy has been reported to be around 20% in the Japanese population [6].
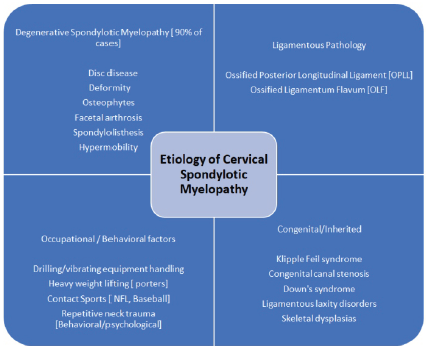
Other factors, which also contribute to the etiological spectrum of the CM, include clinical syndromes, skeletal dysplasia, and connective tissue disorders associated with ligamentous laxity. Klippel Feil syndrome is commonly associated with sub-axial CM. Down’s syndrome usually presents with craniocervical junctional myelopathy due to associated C1-C2 subluxation. Ligamentous laxity disorders, such as the Ehlers Danlos syndrome, and epiphyseal dysplasia, though uncommon, have a high incidence of CM. Overall, congenital and inherited cases comprise around 3-4% of the total CM cases [1].
PATHOPHYSIOLOGY, CLINICAL FEATURES and INVESTIGATIONS
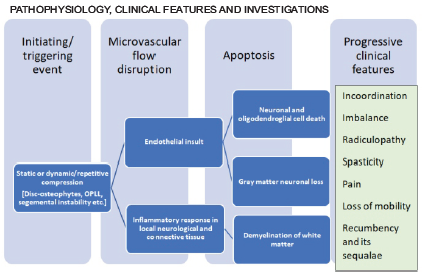
Even though the exact pathophysiology is unclear, the primary insult seems to be a disruption in the microvascular flow of the spinal cord. This disruption could be due to repetitive dynamic compression or continuous static pressure. It activates the endothelium mediated inflammatory cascade, which is hypothesized to trigger apoptosis in the neural and glial tissue — this cascade results in the disruption of axonal flow in long tracts of the spinal cord [2]. The most common presenting complaints are gait imbalance and fine muscle incoordination. More advanced cases present with significant spasticity and are usually not independent walkers.
Magnetic resonance imaging (MRI) remains the mainstay for the identification of cord signal changes such as myelomalacia and to define the extent of compression. In cases of OPLL and OLF, a computerized tomographic (CT) scan will delineate the pattern and extent of ossification. Standard cervical lateral radiographs are crucial for the assessment of cervical lordosis and to guide the choice of surgical approach. Dynamic lateral cervical radiographs can be helpful to identify preexisting instability.
SURGICAL MANAGEMENT

TREATMENT OPTIONS:
Non-surgical treatment is not usually successfull once the patient develops myelopathic symptoms. Myelopathy makes ambulation difficult, and even trivial slips and falls may put one at the risk of sudden deterioration in neurological status. Surgical treatment not only arrests further neurological deterioration but can also improve the symptoms of myelopathy.
The primary goal of surgical treatment is to provide the spinal cord relief from compressive elements. Anterior procedures such as discectomy or corpectomy with fusion are relatively more powerful in achieving lordosis. They are designed to remove the cause of compressive insult and are helpful in cases where compression is present in a kyphotic alignment or when a disc-osteophyte complex is causing primarily anterior compression at 1 or 2 levels.
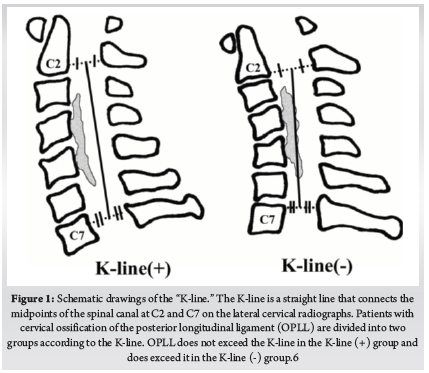
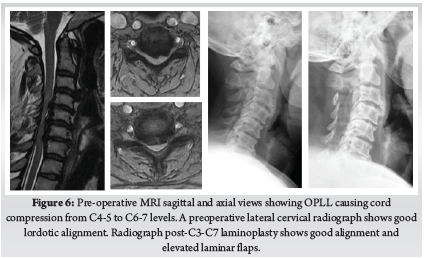
When the compression is due to OPLL, or when 3 or more levels are involved in disc-osteophyte complexes- a posterior indirect decompression in the form of a laminectomy/laminoplasty with fusion or a laminoplasty provides better outcomes. Laminoplasty is associated with a better range of movement compared to the fusion procedures but has been reported to have an increased incidence of neck pain. There is considerable evidence to indicate that the laminoplasty has reduced complication and re-operation rates compared to anterior surgery for CSM involving three or more levels. However, for the laminoplasty to be successful, lordotic cervical alignment is an absolute pre-requisite for the cervical cord to “spring back” away from OPLL. The K-line is an important tool to determine the feasibility of a laminoplasty [6]. When the compression is anterior to K-line (K line +), posterior decompression surgery is often recommended for OPLL patients to avoid the risks involved in multilevel anterior corpectomy. (Fig. 1)
In cases of severe long-standing compression, postoperative worsening of neurological status can be seen, sometimes, despite adequate decompression. It is probably related to rebound cord edema following sudden cord decompression, especially in a long-standing compression. Patients and relatives must be made aware of this catastrophe during pre-operative counseling. The benefits of surgery can only be optimized if a structured post-operative physical and occupational rehabilitation program is implemented.
Anterior Cervical Approach:
The anterior cervical approach described by Smith and Robinson in the 1960s, utilizing the natural anatomical corridor between the carotid vascular bundle laterally and tracheo-esophageal complex medially, has remained the standard route of access for most anterior cervical surgeries. This corridor can be safely traveled upon to approach the spine from C2-C3 disc space to C7-T1 disc space in most individuals. Even though there is some risk of injury to the recurrent laryngeal nerve through the right-sided approach, it is an infrequent complication. Thoracic duct injury on the left side is even rarer. We take an approach contralateral to the side of the symptoms/compression to aid direct – end-on- visualization of the compressive pathology. In cases where the compression is central, and both the sides are equally affected, we utilize the right-sided approach, which is the preferred approach of most right-handed surgeons.
Anterior Cervical Discectomy and Fusion:
The anterior cervical discectomy and fusion remains one of the most rewarding procedures in the spine surgery repertoire. Initial reports of anterior cervical discectomies did not incorporate bone grafting, which was subsequently introduced and popularized by Cloward, Smith, and Robinson. Plate and screw systems to stabilize the graft and aid the fusion have gone through several generations of design over the last few decades. There is evidence to suggest that the plate fixation is superior in terms of fusion rate and graft subsidence compared to non-instrumented fusion [7]. Though the consensus about the value of strut autografts vs. cages, titanium vs. PEEK, and whether to plate or not is still not achieved, anterior cervical discectomy and fusion with plating has become a standard of care in the treatment of various cervical pathologies.
Our preferred skin incision is the horizontal one utilizing natural skin creases. Skin marking can be done with needles or superimposed k-wires under c-arm guidance. Up to 3 disc spaces can be easily accessed in this fashion, and the resulting scar is cosmetic and usually avoids the hypertrophic reaction observed in the vertical incision. The platysma is then incised parallel to the skin incision. Though scissors are a useful tool to separate the platysma from the underlying fascia and incise it, the use of electrocautery can minimize the bleeding at this stage. Utilization of an artery forceps to elevate the muscle from underlying tissues is helpful while using the electrocautery.
Deeper to the platysma, the medial border of the bulk of the sternomastoid muscle defines the lateral extent of the approach. This landmark is usually easily identifiable even in revision exposures. Dissection from here onwards is performed with blunt instruments such as cotton sponges on forceps or with fingertips. The bulk of omohyoid can be encountered around the C5 level, which is identified and resected. Carotid pulsations are then palpated to locate the carotid bundle. Loose areolar tissue between the carotid bundle and the tracheal rings usually guides the surgeon’s finger to the center of the cervical spine. During the early part of the learning curve, it is crucial to guide the finger more medially if the bony cervical spine is not adequately felt. It is vital to make sure that the assistants holding the retractors, especially over the carotid bundle, are not applying too much pressure. Large bleeders can be cauterized or ligated with clips/sutures if need be. Thyroid vessels can be encountered during the exposure, and we prefer to use clips to ligate them.
Once over the bone, medial borders of longus colli are identified. Medial edges of the longus colli can be elevated with bipolar electrocautery to determine the upward rise of the uncovertebral joints, which demark the boundary of the lateral dissection. The glistening peaks are the discs, while the vertebral bodies form the valleys in between the peaks. A check shoot for the level is then taken with a bayonet- shape bent k wire.
It is essential to maintain a subperiosteal plane while elevating the longus colli muscles as cervical sympathetic trunks run vertically along the lateral aspect of the muscle. Horner’s syndrome can be encountered if the sympathetic trunks are damaged during the dissection. Maintaining a subperiosteal plane ensures that the recurrent laryngeal nerve (RLN) is retracted with the longus colli muscle. This is especially important while performing a right-sided approach as the right RLN has a variable course and lies more anterior and lateral compared to the left.
One has to be extremely careful about the esophageal musculature- thicker than the adjacent soft tissue- jutting out from under the retractors. The Ryle’s tube is invaluable in identifying the esophagus intra-operatively and preventing esophageal injuries, especially during revision exposures.
Discectomy is carried out in the usual fashion by incising the annulus. The use of a small osteotome or a periosteal elevator facilitates the removal of the degenerated disc from the endplates. Once sufficient discectomy is performed, a Caspar pin retractor is inserted. It is essential to keep the pins in midline and parallel to the endplates. This position serves as a guide to the midline of the spine during surgery and keeps the passage of the retractor pins away from the trajectories of the screws. The parallelism of the pins will provide an optimal distraction while performing the decompression. While we recommend the Caspar pin retractor for the vertical retraction, we prefer the handheld retractors for the retraction of the trachea-esophagus and the carotid bundle. Our experience agrees with the published reports of reduced postoperative dysphagia with the use of handheld retractors8.
The posterior part of the disc is removed with rongeurs till the posterior longitudinal ligament (PLL) is exposed. It is seen as glistening vertically arranged fibers distinct from the circular whitish tissue of the annulus. If it is ossified, then a burr is used to thin the bone, which is subsequently punched off with a size 1 or 2 Kerrison’s rongeur. A midline cleft is usually separable in the healthy PLL, which can be identified and resected laterally till the uncovertebral joints. Dura is recognized as a transparent white sac with epidural vasculature. Foraminotomies are performed with rongeurs as needed. Bleeding from the foramen is usually an indirect indication of decompression. End plates are then prepared to the bleeding subchondral bone with curettes and burrs. Care must be taken not to remove too much subchondral bone while endplate preparation to avoid cage or bone graft subsidence.
After sizing, which can be done with the sizers provided in the implant systems or graduating size of osteotomes, appropriate size bone graft strut or cage is kept in the disc space. If utilizing a bone-graft strut, it is imperative to shape it to the disc space with the use of saws and rongeurs.
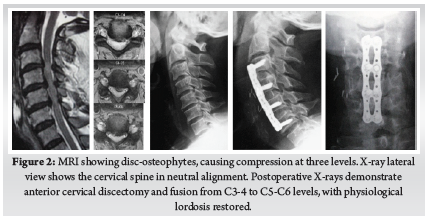
A plate of appropriate size is chosen and stabilized with screws. Various systems offer different screw types, but our preference is to use blunt-tipped, manually drilled, and self-tapping variable angle screws. Screws must converge medially and ideally should stop just short of the posterior cortex. Screws of 14 or 16 mm length are usually sufficient for patients from the Indian subcontient. Screws are directed slightly divergent, toward the subchondral bone of the endplates. (Fig. 2)
Anterior Cervical Corpectomy and Fusion:
For a cervical corpectomy, the discectomy is performed at the above, below, and the intermediate levels first. Subsequently, the vertebral body is removed with rongeurs or burrs. We use a harmonic bone scalpel, which reduces the bleeding significantly and preserves a good quantity of bone for subsequent grafting. The posterior wall is removed with Kerrison’s rongeurs and burrs till the dural sac is visible. Corpectomies tend to bleed significantly at this stage, and having an efficient hemosealant such as Surgiflo [© Johnson & Johnson Medical N.V., Belgium] helps achieve rapid hemostasis. Uncovertebral joints demark the lateral boundaries of the corpectomy defect.
In some instances, the dura is also involved in the ossified mass and is often adherent to the ossified PLL or the disc-osteophyte complexes. In such cases, removal of total ossified mass can result in an unintentional dural injury. We usually resort to the floatation technique for such cases. The ossified mass is thinned out with a burr. The edges of the mass are then made free of the surrounding dura till the adherent dura can no longer be separated with a small nerve hook or a small dural elevator. The resultant adhered island is then left to float surrounded by decompressed dura. This technique provides adequate decompression to the cord and avoids complications due to inadvertent dural injury.
Multiple options are available for the stabilization of the corpectomy defect. Our preference is to use a titanium mesh cage filled with locally harvested bone graft, which is buttressed with an anterior cervical plate and screw construct. Reshaping the cage to provide it a lordotic shape ensures the stability after insertion. Care must be taken while positioning the cage or bone graft strut to ensure that it is not pushed too posterior. Careful measurement, using cage punches with a flange towards the adjacent intact vertebra, ensures that the cage will not be pushed too far back. The use of a burr to flatten the anterior osteophytes can be helpful to make the plate sit flush on the spine. In certain cases, when two or more levels corpectomy is performed, we prefer to augment the construct with posterior stabilization and fusion.
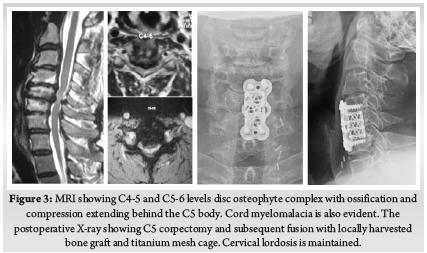
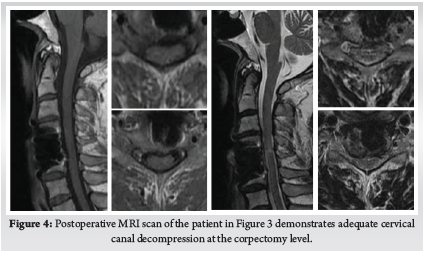
Careful cauterization of the bleeders and bone surfaces is a must to prevent postoperative hematoma, especially in corpectomy. We prefer bone wax to plug the oozing bony surfaces and Surgiflo [© Johnson & Johnson Medical N.V., Belgium] to control the soft tissue bleeders. A drain is kept before closing the wound in layers. We use absorbable stitches for the skin and bone graft site closure. A soft collar can be used post-operatively for a few weeks to aid soft tissue healing. (Fig. 3) (Fig. 4)
Posterior Surgical Procedures:
The posterior approach to the cervical spine is essentially a continuation of the midline subperiosteal corridor, which can be accessed from sacrum to occiput. However, there are a few caveats to ensure the safety of the approach and optimize the exposure. C2-C6 cervical spinous processes are bifid, and the C7 is the first non-bifid spinous process. The ligamentum nuchae is usually tortuous in its length to accommodate the lordosis. It is important to follow its course to access the median avascular plane. Keeping the head in a slightly flexed or neutral position makes the ligament taught and facilitates the identification of the avascular plane. An effort is made to preserve the muscle attachments at the tip of the C2 spinous processes to minimize postoperative pain and kyphosis.
In the case of laminoplasties, the exposure can be limited to the spino-laminar junction to preserve the integrity of the facet capsules. If fusion is planned, the dissection is taken laterally to the facet joints. One must not go lateral to the facet joints to avoid injuring the vertebral artery.
Cervical Laminectomy and Fusion:
While positioning the myelopathy patient for laminectomy and fusion, it is advisable to keep the neck in a neutral or slight kyphotic alignment to ensure adequate space for the compressed cord while positioning. We prefer to put the lateral mass screws before the laminectomies. A point at the infero-medial aspect of the center of the lateral mass is first decorticated with a burr. A measured and calibrated drill bit with stop-lock is then utilized until the opposite cortex is pierced. A practical guide for maintaining alignment is to rest the drill bit on the spinous process of the inferior vertebra. This maneuver guides the drill parallel to the plane of the facet joint and is coaxial to the center of the lateral mass. Alternatively, a small blunt k-wire can be inserted in the facet joint for recognizing the orientation of the plane of the joint. Self-tapping or manually tapped screws can be utilized.
For the subsequent laminectomy, we prefer a burr to remove the dorsal cortex of the laminae. Once the glassy cortex of the anterior aspect is visualized, a size 1 or 2 Kerrison rongeur is utilized to complete the laminectomy. When available, a harmonic bone scalpel can be used to perform a safe through and through laminectomy. Foraminotomies are done as needed by removing the bone carefully with a size 1 or 2 Kerrison punch. Profuse bleeding can be encountered while doing foraminotomies and can be controlled with the use of patties or hemosealants.
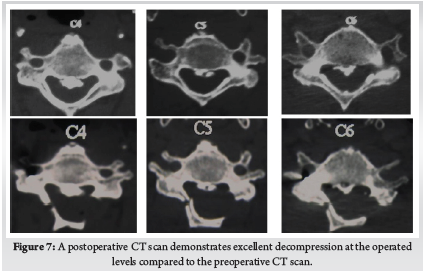
Once the laminectomy is complete, lordosis is restored by repositioning the neck in extension, and the alignment is maintained with the help of contoured rods and lateral mass instrumentation. Facet joints and exposed bone surfaces are then decorticated with a burr, and a morselized local autograft is applied. We prefer to put a collagen sponge on the exposed dural surfaces to prevent postoperative adhesions. Bleeding surfaces and points are cauterized to minimize the postoperative hematoma. The wound is closed in the usual fashion over a drain. A soft cervical collar can be utilized for a few weeks to aid soft tissue healing. (Fig. 5)

Posterior Cervical Laminoplasty:
Described first by Hirabayashi in 1981, the cervical laminoplasty has progressively gained popularity [9]. The aim of the cervical laminoplasty is to preserve the facet joints while providing adequate decompression. This goal is achieved by creating a unicortical hinge in the laminae on one side as in the open door laminoplasty or on both the sides – also known as the French door laminoplasty. Subsequently, the decompression is achieved by elevating a laminar flap to one side or from both sides, allowing the spinal cord to spring-back posteriorly [6].
We use the open-door approach. The laminectomy is usually done on the side of the radiculopathy symptoms or on the right side for the right-handed surgeons. A laminoplasty trough is first prepared by removing the dorsal cortex with a 5 mm burr till the glassy surface of anterior cortex is visible. Then, the laminectomy is performed on the opposite side. In most cases, the laminoplasty is performed at C3-C6 levels, and the C2 lamina is decompressed in a dome fashion. Depending on the extent of compression, the upper edge of the C7 lamina can be similarly cut in a dome fashion. Once the trough and the laminectomy are done, the laminae are gradually elevated with a small osteotome till they open up at the hinge.
Once the laminar flaps are elevated, the resulting gap at the laminectomy sites – or the midline cleft in case of French door laminoplasty- must be maintained. Various implant systems with multiple options of spacers are available. We use an uninstrumented variant developed by us to keep the gap open and provide support for the hinge to heal. A non-absorbable polyester suture material such as Ethibond [© Johnson & Johnson Medical N.V., Belgium] is used to keep the laminar flaps elevated10. The wound is closed over layers and a drain is kept. A soft cervical collar can be used for a few weeks to aid soft tissue healing.
Inadvertent laminectomy can happen while creating the trough or while elevating the laminoplasty flap, and one must be prepared to convert the procedure into a laminectomy and fusion with the necessary toolset. Post-operative neck pain can complicate the laminoplasties; thus, a laminectomy with fusion is a better alternative in cases with considerable pre-operative neck pain. Post-operative C5 palsy can complicate both the laminectomy and laminoplasty and can be a frustrating complication. However, most of the C5 palsies recover over time11.
Cervical Laminoplasty and fusion:
The combination of laminoplasty and instrumented fusion can be utilized as an alternative to laminectomy and fusion. We prefer this hybrid procedure in cases where the local cervical kyphosis can be brought to neutral or in some lordosis but not sufficient enough for a standard laminoplasty, or there is evidence of some segmental instability. In these cases, the laminoplasty is performed in the usual manner. The facets are then decorticated with a burr in the typical fashion, and locally-harvested graft is applied with lateral mass instrumentation for the fusion. The laminectomy gap and the elevated laminar flaps are kept in situ as in a standard laminoplasty.
This hybrid technique is reported to have several advantages. Natural cover provided by the laminae prevents the adherent scar formation seen in open laminectomies. Fusion can be augmented by using the decorticated dorsal laminar surfaces to provide an enhanced bed for the bone graft. Posterior tension band can be preserved, which can promote faster healing and result in less post-operative pain [12]. (Fig. 6) (Fig. 7)
Uniform Precautions for Surgical Management of Myelopathic Patients:
1. Awake fiberoptic intubation is a necessity for these patients as hyperextension of the cervical spine during routine intubation can result in deterioration of neurology.
2. Communicate with the anesthesia team for keeping the mean arterial pressure above 75-80 mmHg throughout the procedure. Ensure the presence of an anesthesiologist monitoring the vitals while positioning the patient; especially during the decompression.
3. A Ryle’s tube is a must for any anterior cervical procedure. It makes it safer to retract the esophagus and is indispensable while identifying the esophagus in the operative field.
4. While positioning the patient for ACDF/ACCF, care must be taken to ensure the neutral or slightly lordotic curvature. Hyperextension of the cervical spine must not be done to prevent the worsening of neurology. Bunching up of spinous processes on a lateral c-arm shot is an indicator of excessive extension.
5. Mayfield’s clamp or a similar three-point fixation device is a must for posterior surgeries. Care must be taken not to hyperextend/ twist the neck while turning the patient.
6. The neck is kept in the neutral or a slightly flexed position during the beginning of posterior surgery to facilitate muscle exposure and posterior decompression. In cases where fusion is planned, the neck is extended to achieve adequate lordosis after the decompression and prior to instrumentation.
7. Intra-operative neuromonitoring, when available, should be utilized.
Outcomes of Cervical Myelopathy:
Various measures for the outcome assessment in cervical myelopathy have been devised. The modified Japanese Orthopedic Association score (mJOA) is one of the most common assessment tools. The mJOA includes functional scores for both the upper and lower extremities, sensory and bladder functions, and includes categories for significant functional impairment. The mJOA provides numerical scoring and divides the outcome in mild 15-17, moderate 12-14 and severe <12 categories. It has been validated across various languages and is readily available online. The Nurick grading is a more straightforward and valid tool to assess functional impairment with regards to mobility and employment status. The patient’s functional impairment is categorized into six separate strata. The grade zero cases have only root level involvement, while progressive spinal cord involvement and consequent occupational and mobility impairment are graded from I to V; with a grade V case being chair bound or bedridden. The Nurick grade does not include the granular level assessment as the mJOA but provides rapid insight into the impact of myelopathy in patient’s activities of daily living. Other indices, such as the SF-36v2, the neck disability index and 30-meter walking test, have also been reported. The 30-meter walking test is a rapid and effective tool distinguishing controls from myelopathic patients [13].
For the patients undergoing surgical treatment, positive predictors of outcomes include younger age at presentation, shorter duration and mild severity of preoperative symptoms, lack of smoking history, absence of psychiatric disorder, and normal gait at initial presentation [14]. There is low level evidence to suggest that greater number of segments with greater signal intensity (SI) changes in T2-weighted images (WI), low change on T1WI signal intensity, and a higher T1/T2 SI ratio favor irreversible changes in cord histology and predict worse outcomes in postoperative period. However, isolated high grade T2SI change, canal compression ratio and absolute canal diameter are not reported to be predictive of surgical outcomes [15]. Newer imaging modalities such as the diffusion tensor imaging and tractography, functional MRI and MR spectrography are being investigated for their prognostic potential [13]. However, the surgical decision making must be focused on patient’s symptoms and functional impairment with the imaging serving as diagnostic aid.
Summary:
Cervical spondylotic myelopathy (CSM) is a surgical disease, and early intervention is rewarded with better outcomes. Anterior cervical procedures are ideal for disc-osteophyte complexes involving one or two levels or in a kyphotic cervical spine. Laminoplasty is a motion preserving option for patients with adequate cervical lordosis without significant neck pain. Posterior cervical laminectomy or laminoplasty with fusion provide optimal indirect decompression and pain relief in cases with OPLL who have significant neck pain and lordotic or neutral sagittal alignment. Posterior surgery has reduced complication rates for CSM involving three or more levels.
References
1. Yamaguchi S, Mitsuhara T, Abiko M, Takeda M, Kurisu K. Epidemiology and Overview of the Clinical Spectrum of Degenerative Cervical Myelopathy. Neurosurg Clin N Am. 2018;29(1):1-12. doi:10.1016/j.nec.2017.09.001
2. Karadimas SK, Gatzounis G, Fehlings MG. Pathobiology of cervical spondylotic myelopathy. Eur Spine J Off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc. 2015;24 Suppl 2:132-138. doi:10.1007/s00586-014-3264-4
3. Wu J-C, Ko C-C, Yen Y-S, et al. Epidemiology of cervical spondylotic myelopathy and its risk of causing spinal cord injury: a national cohort study. Neurosurg Focus. 2013;35(1):E10. doi:10.3171/2013.4.FOCUS13122
4. Joaquim AF, Hsu WK, Patel AA. Cervical spine surgery in professional athletes: a systematic review. Neurosurg Focus. 2016;40(4):E10. doi:10.3171/2016.1.FOCUS15560
5. Reddy KVS, Mudumba VS, Tokala IM, Reddy DR. Ossification of posterior longitudinal ligament and fluorosis. Neurol India. 2018;66(5):1394-1399. doi:10.4103/0028-3886.241343
6. Fujiyoshi T, Yamazaki M, Kawabe J, et al. A new concept for making decisions regarding the surgical approach for cervical ossification of the posterior longitudinal ligament: the K-line. Spine. 2008;33(26):E990-993. doi:10.1097/BRS.0b013e318188b300
7. Oliver JD, Goncalves S, Kerezoudis P, et al. Comparison of Outcomes for Anterior Cervical Discectomy and Fusion With and Without Anterior Plate Fixation: A Systematic Review and Meta-Analysis. Spine. 2018;43(7):E413-E422. doi:10.1097/BRS.0000000000002441
8. Mendoza S, Clifford K, Bartelt R, Stewart J, Clark C, Boezaart A. Dysphagia following anterior cervical arthrodesis is associated with continuous, strong retraction of the esophagus. J Bone Joint Surg Am. 2008;90:256-263. doi:10.2106/JBJS.G.00258
9. Hirano Y, Ohara Y, Mizuno J, Itoh Y. History and Evolution of Laminoplasty. Neurosurg Clin N Am. 2018;29(1):107-113. doi:10.1016/j.nec.2017.09.019
10. Dhillon CS, Ega SR, Tantry R, et al. Outcome Evaluation of Modified Uninstrumented Open-door Cervical Laminoplasty for Ossified Posterior Longitudinal Ligament with Cervical Myelopathy. Indian J Orthop. 2019;53(4):510-517. doi:10.4103/ortho.IJOrtho_207_19
11. Pan F-M, Wang S-J, Ma B, Wu D-S. C5 nerve root palsy after posterior cervical spine surgery. J Orthop Surg Hong Kong. 2017;25(1):2309499016684502. doi:10.1177/2309499016684502
12. Bridges KJ, Simpson LN, Bullis CL, Rekito A, Sayama CM, Than KD. Combined Laminoplasty and Posterior Fusion for Cervical Spondylotic Myelopathy Treatment: A Literature Review. Asian Spine J. 2018;12(3):446-458. doi:10.4184/asj.2018.12.3.446
13. Wilson JR, Tetreault LA, Kim J, et al. State of the Art in Degenerative Cervical Myelopathy: An Update on Current Clinical Evidence. Neurosurgery. 2017;80(3S):S33-S45. doi:10.1093/neuros/nyw083
14. Tetreault LA, Côté P, Kopjar B, Arnold P, Fehlings MG, AOSpine North America and International Clinical Trial Research Network. A clinical prediction model to assess surgical outcome in patients with cervical spondylotic myelopathy: internal and external validations using the prospective multicenter AOSpine North American and international datasets of 743 patients. Spine J Off J North Am Spine Soc. 2015;15(3):388-397. doi:10.1016/j.spinee.2014.12.145
15. Tetreault LA, Dettori JR, Wilson JR, et al. Systematic review of magnetic resonance imaging characteristics that affect treatment decision making and predict clinical outcome in patients with cervical spondylotic myelopathy. Spine. 2013;38(22 Suppl 1):S89-110. doi:10.1097/BRS.0b013e3182a7eae0
| How to Cite this Article: Dhillon CS, Chhasatia N| Surgical Management of Cervical Myelopathy: Current Algorithm| International Journal of Spine| January-June 2023; 8(1): 11-17. |
(Full Text HTML) (Full Text PDF)
Vestigial Tail Associated to Spinal Lipomas: Report of Seven Cases
Volume 8 | Issue 1 | January-June 2023 | Page: 07-10 | Arce-Lozoya Mayra Alejandra, Ramírez-Reyes Alma Griselda, Arredondo-Navarro Luis Ángel, Rajendra Sakhrekar
DOI: https://doi.org/10.13107/ijs.2023.v08.i01.45
Submitted: 09/04/2023; Reviewed: 26/04/2023; Accepted: 09/05/2023; Published: 10/06/2023
Authors: Arce-Lozoya Mayra Alejandra [1], Ramírez-Reyes Alma Griselda [1], Arredondo-Navarro Luis Ángel [2], Rajendra Sakhrekar [3]
[1] Department of Pediatric Neurosurgery, UMAE Hospital, Siglo XXI, CdMx, México.
[2] Department of Pediatric Neurosurgery, Hospital Civil Fray Antonio Alcalde, Guadalajara, Jalisco, México.
[3] Department of Orthopaedics, The Hospital For Sick Children, Toronto, Canada.
Address of Correspondence
Dr. Arce-Lozoya Mayra Alejandra
Department of Pediatric Neurosurgery, UMAE Hospital, Siglo XXI, CdMx, México.
E-mail: mayra.arce.lozoya@gmail.com
Abstract
Objective: Vestigial tail is a rare form of cutaneous stigmata often related to occult spinal dysraphism. We present 7 cases of vestigial tail associated to tethered cord and spinal lipomas in the Pediatric Neurosurgery Service of the Hospital Civil de Guadalajara.
Methods: In this retrospective study from 2017-2022 we reviewed the spinal dysraphism data base of the Hospital de Guadalajara and included the cases of vestigial tails.
Results: 7 patients, 5 female and 2 males with vestigial tails were included. Six different morphologies of tails are described so as their location and relationship to occult spinal dysraphism. All the patients received surgical treatment. Complete resection of the cutaneous stigmata and cord detethering were performed in four cases related to fatty filum terminale and the remaining three of the patients required radical resection of associated complex conus medullaris lipomas. All the surgical procedures were performed with microsurgical techniques and neurophysiological monitoring.
Conclusions: The different classifications include two main forms of tails, true tail and false tail. Most true tails represent only a cosmetic issue, while the false ones are often in close relationship with spinal dysraphism. Considering the risk of underlying malformations associated with false human tails, the preoperative assessment should include a thorough neurological examination, and a spine magnetic resonance imaging. We present the association of several forms of spinal lipomas related to vestigial tails.
Keywords: Vestigial tail, Tethered cord, Spinal lipoma, Pseudo tail, Occult spinal dysraphism.
Introduction
Occult spinal dysraphism (OSD) is commonly characterized by skin-covered lesions mainly localized in the lumbosacral area. As skin and nervous tissue are of ectodermal origin, anomalies of both may occur at the same time [1]. Vestigial tails (VT) are rare and heterogenic forms of cutaneous stigmata and might be related to different forms of tethered cord (TC) and OSD.
Most of the knowledge related to VT comes from case reports, thus large series are unavailable. Many descriptions and classifications have merged since Bartles first described it in 1884. Harrison in 1901 made the first differentiation amongst the true and the false tail, naming the nonbony lesion as “caudal appendage”. Since then, various authors presented their different classifications until Dao and Netsky in 1984, published their classical description of “true human tail” and “pseudo tail” which is grossly still in use nowadays [2, 3].
Based on these descriptions, “true tails” include vertebrae, although their embryological origin is different than the false or vestigial tails. VT are different forms of appendages covered by skin and mainly composed of mesenchymatous tissues including fibrous, adipose, and sometimes striated muscle. Nerves can be observed in pathological specimens. These VT are associated with OSD in some cases [3] and represent a major risk to develop a TC syndrome while the child grows up [4].
The report of different forms of spinal lipomas and cord TC in association to VT is not often found in the current literature, we present though 7 cases of VT associated to a different variety of spinal lipomas and TC in the Pediatric Neurosurgery Service of the Hospital Civil de Guadalajara, México.
This case report has been reported in line with the SCARE Criteria [10].
Material and Methods
We reviewed the spinal dysraphism data base of The Hospital Civil de Guadalajara from 2017 to 2022 and selected 7 cases of vestigial tail: 5 female and 2 males. The archives included clinical photos and study images along with the clinical charts. An informed consent was achieved from each of the cases and the identity of the patients was preserved under the regulations of good medical practices. A Magnetic Resonance Imaging assessment was performed in each of the patients. All the patients were operated on for resection of the VT and for the different OSD under microsurgical techniques and neurophysiological monitoring. The morphology and location of the VT were classified according to Tojima and Yamada classification 2020 [2].
Results
Seven patients with several forms of vestigial tails were included and analyzed. Demographic data, morphology and location of the tail, clinical findings, type of surgical procedure, type of dysraphism associated and follow up are shown in table 1.
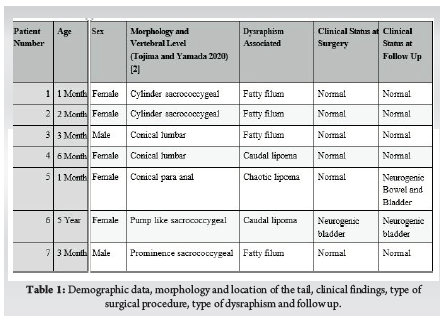
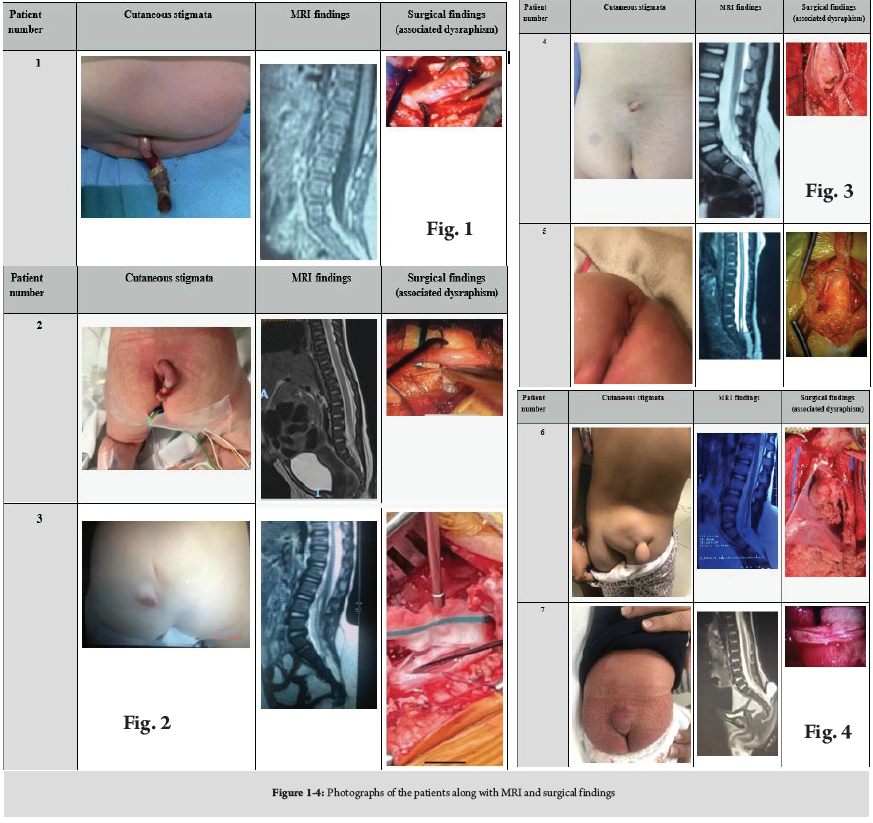
A total of 7 patients were included, 5 female and 2 males; the age range was 1 month old to 5 years old, with a median of 3 months. The aspect of cutaneous stigmata was remarkably heterogeneous varying from tail shaped lesions (cases 1 and 2) to appendicular lesions (cases 3, 4, 5, 6, 7) All of the cases had a preoperative MRI, the lower conus medullaris position below the L2-L3 transition was common in all the cases, a fatty filum terminale was observed in 4 cases (patients 1, 2, 3 and 7), and lipomas of the conus medullaris in three, 1 transitional chaotic lipoma (patient 5) and two caudal lipomas (patients 4 and 6). The clinical preoperative status was normal in almost all the cases, patient 6 had neurogenic bladder though. All the patients were operated on under microsurgical technique and strict neurophysiologic monitoring. Findings during surgery corresponded to preoperative MRI. The postoperative clinical follow up remain unchanged in patients 1, 2, 3, 4, 6, 7 and patient 5 developed neurogenic bladder during her growth (Fig. 1-4).
Discussion
VT are rare embryonic anomalies occurring in the lumbar, sacrococcygeal and peri anal regions. Covered in skin, these lesions are mostly pseudo tails and have an enhanced relevance due to its association to several forms of OSD. On the other hand, the true tails include bone and resemble more to those present in other non-human vertebrates [2, 9]. VT probably occur during the 5th and 6th gestational week and this represent their common association to OSD and TC.
Many attempts to classify this anomaly have being used throughout the times and are cited in most of the papers referring these cases [2, 8]. Most of classifications of the so called “true” or “false” tails are based on the presence of bone, calling “true tails” to those bonny appendages. Although the reports of true tails composed of bony elements are extremely rare (counting just a few cases described) may still causing confusion now to establish a fine description [11]. It is important to establish that VT or pseudo tails are more often related to an OSD and must be considered under the spectrum of cutaneous stigmata requiring a more accurate screening of the patients. Thus, in the strict sense, the description of a true tail must not be confused with a VT in terms of treatment, assessment and follow up [11].
We found the classification made by Tojima and Yamada in 2020 very useful. They described three main anatomic locations and six shapes of the vestigial tails. In our point of view this is a simple and accurate way to classify the lesions [2, 3].
In this paper we present the association of different spinal lipomas in all the cases. Four filar lipomas and three lipomas of the conus medullaris, according to the several classifications for spinal lipomas [5] Spinal lipomas are not simple lesions and require a vast experience of the surgeon to treat them, especially in cases of those of the conus medullaris [6].
We found no reports of transitional chaotic lipomas associated to peri anal vestigial tails, as we found in the case number five; so, this might be considered in the assessment of patients with these anomalies. The development of neurogenic bladder in this case could be related more to the type of spinal lipoma she presented, rather than the result of the surgical procedure. Chaotic lipomas are associated to an uncertain prognosis no matter the moment the surgery is performed [6].
The four filar lipomas were completely excised, along with the correction of the cutaneous tail. In the more complex conus medullaris lipoma cases, an aggressive radical resection was attempted to remove most of the lipoma, in two cases the placode neurulation was feasible.
The seven cases we present are of utmost interest because we encountered a very strong relationship of VT to different forms of spinal lipomas. If we referred to the embryonic classification of these lesions, Morota et al. published a brand-new classification of spinal lipomas according to embryonic stage [5]. All our patients presented some different forms of spinal lipomas, 4 fatty filum terminale, 2 caudal lipomas and 1 chaotic lipoma. This finding probably can lead us to realize if there is a relationship between the cutaneous stigmata and the subjacent OSD according to the embryonic stage, and may be important to encourage the need for a complete screening of the spinal cord rather than the simple cosmetic resection of the VT.
We emphasize the importance of the risk of underlying spinal lipomas and tethered cord associated to these vestigial tails. Several other reports have mentioned the associations of dermal sinus and other forms of OSD [7]. Dermal sinus tract is as well a very concerning OSD due to the association of spinal cord dermoid cysts.
The presence of a VT is a matter of concern for the parents, so they might feel under pressure for their child to be operated on as soon as possible. The timing is important for removing the VT and the decision to treat the underlying OSD must be as important as well, thus a thorough assessment since the initial visual diagnosis, must be completed with the appropriate studies, in order to establish the definitive treatment.
The correct recognition of an OSD and its prompt treatment, could be of benefit in preventing future neurologic, orthopaedic or urologic disorders; nevertheless, the early treatment of asymptomatic patients with tethered cord is still on debate and further studies are needed.
Conclusions
1. Most of true tails represent only a cosmetic issue
2. Pseudo-tails are often related to spinal dysraphism.
3. Considering the risk of underlying malformations associated with human tails, the preoperative assessment should include a thorough neurological exam, plain radiographs to clear spinal defects and a spine magnetic resonance imaging.
4. Surgery in these cases should be focused in untethering the cord and the esthetical correction of the cutaneous stigmata.
References
1. Guggisberg D et al. Skin markers of occult spinal dysraphism in children. A review of 54 cases. Arch Dermatol 2004;140:1109-115.
2. Tojima S, Yamada S. Classification of the “human tail”: Correlation between position, associated anomalies, and causes. April 2020 Pages 929- 942.
3. Rueda J et al, Human tail in a newborn. Journal of Pediatric Surgery 2022. 102098.
4. Hertzler DA, De Powell JJ, Stevenson CB, Mangano FT. Tethered cord syndrome: a review of the literature from embryology to adult presentation. Neurosurg Focus 29(1):E1, 2010.
5. Morota N, Ihara S, and Ogiwara H. New classification of spinal lipomas based on embryonic stage J Neurosurg Pediatr 19:428–439, 2017.
6. Pang D. Management of complex spinal cord lipomas: a new perspective. J Korean Neurosurg Soc. 2020 May; 63(3) 279-313.
7. Mukhopadhyay B, et. Al. Spectrum of human tails: A report of six cases J Indian Assoc Pediatr Surg. 2012 Jan-Mar; 23–25.
8. Wilkinson CC, Boylan A. Proposed caudal appendage classification system; spinal cord tethering associated with sacrococcygeal eversion. In Child’s Nervous System Ausgabe 2017.
9. Turk CC, Kara NN, Bacanli A. The human tail: a simple skin appendage or cutaneous stigma of an anomaly?. Turk Neurosurg. 2016;26:140-5.
10. Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A. The SCARE 2020 Guideline: Updating Consensus Surgical CAse REport (SCARE) Guidelines .International Journal of Surgery. https://doi.org/10.1016/j.ijsu.2020.10.034.
11. Pillai MK, Nair ST. A true human tail in a neonate. Case report and literature review. Sultan Qaboos University Med J, February 2017, Vol. 17, Iss. 1, pp. e109–111.
| How to Cite this Article: Arce-Lozoya M A, Ramírez-Reyes A G, Arredondo-Navarro L Á, Sakhrekar R | Vestigial Tail Associated to Spinal Lipomas: Report of Seven Cases | International Journal of Spine | January-June 2023; 8(1): 07-10. |
(Full Text HTML) (Full Text PDF)
Efficacy of Transforaminal Steroid Block for Pain Relief Due to Recurrent Lumbar Disc Herniation in Previously Operated Case of lumbar Discectomy
Volume 8 | Issue 1 | January-June 2023 | Page: 01-06 | Chandrasen Chaughule, Nitin Bhalerao, Anjaney Karangutkar, Jay Date, Sanket Tanpure, Srishti Tiwari
DOI: https://doi.org/10.13107/ijs.2023.v08.i01.44
Authors: Chandrasen Chaughule [1], Nitin Bhalerao [1], Anjaney Karangutkar [1], Jay Date [1], Sanket Tanpure [1], Srishti Tiwari [2]
[1] Department of Orthopaedics, Dr. Vikhe Patil Medical College, Ahmednagar, Maharashtra, India.
[2] Department of Anaesthesia, Dr. Vikhe Patil Medical College, Ahmednagar, Maharashtra, India.
Address of Correspondence
Dr. Chandrasen Chaughule,
Assistant Professor, Department of Orthopaedics, Dr. Vikhe Patil Medical College, Ahmednagar, Maharashtra, India.
E-mail: csfever10@gmail.com
Abstract
Background: lower Back discomfort as a result of a herniated disc is quite prevalent worldwide, frequently resulting in missed work days and significant changes in affect and motivation. Recurrent lumbar disc herniation is one of the most common problem faced after a lumbar discectomy, most frequently seen among male gender, tall-heighted individuals, heavy workers, obese and smokers. Analgesic and anti-inflammatory medication is the initial course of treatment. But in the majority of instances, it progresses slowly and calls for surgical intervention or minimally invasive treatments like steroid injections.
Aims and Objectives: The purpose of this study is to determine whether transforaminal steroid block can be attempted before surgery for pain relief in cases of recurrent herniated lumbar disc with failed conservative management having intractable radicular pain.
Materials & Methods: Use of transforaminal selective nerve root block (SNRB) in single level recurrent lumbar disc herniation patients was studied. 40 patients with single lumbar disc herniation, operated with discectomy were studied irrespective of age and sex. All patients were injected with a combination of long acting steroid suspension with local anaesthetic (Bupivacaine-plain) near the affected nerve root via cambins triangle approach and the results were analysed.
Result: Those graded mild, were pain free for up to an average of 5.5 months and those graded moderate had 3.3 months of relief. Patients suffering from extensive disc prolapse had immediate post procedural relief but not in long term. 47.5% patients have had a pain free interval upto 6 months.
Conclusion: Transforaminal SNRB is an excellent alternative for pain relief in patients with recurrent lumbar disc herniation having failed conservative management with intractable lumbar radicular pain. It was also found to be a cost effective alternative and relatively less invasive, with almost no complication.
Keywords: Selective nerve root block, Disc prolapse, Recurrent lumbar disc herniation.
Introduction
Recurrent lumbar disc herniation is defined as intervertebral disc herniation at the same level with a pain-free interval of more than six months, regardless of ipsilateral or contralateral herniation. There are several frequent pathologies of the spine, with a lifetime prevalence of 5–18%. In some circumstances, it resolves on its own or with the help of analgesic, anti-inflammatory, and physiotherapeutic therapy; nevertheless, it can also progress chronically with serious negative effects on the mind, society, economy, and quality of life. Transforaminal injections of small doses of steroids have lately been used to alleviate lower back pain, however the condition can become chronic and have severe negative effects on the quality of life. Recently, lower back discomfort brought on by a herniated disc has been successfully treated with transformational injection of modest quantities of steroids [1-6].
In both the cervical and lumbar areas, selective nerve root block (SNRB) is used to treat radicular pain brought on by a specific damaged nerve root [7-9]. Therapeutic efficacy needs to be discussed despite claims that it has a low degree of specificity as a diagnostic tool [10-11]. This modality is being used commonly for those with or without significant surgical spinal lesions [12]. Mechanical lesions include various stages of disc prolapse as in ligamentum flavum hypertrophy, facet hypertrophy and degenerative osteophytes causing foraminal stenosis, all leading to the nerve root irritation [13]. Transforaminal nerve root block has proven to be quite a specific procedure with excellent outcomes in cases of lumbar disc herniation. Being a pain-relieving interventional procedure, it also falls in the purview of different medical care specialists, including spine surgeons, radiologists, anaesthesiologists, and pain physicians, and thus the inclusion criteria and as a result, different studies have quite diverse inclusion requirements and patient evaluation standards. Patients in non-manual job (“white collared”) had a poor outcome with SNRB although studies have revealed a higher incidence of LDH in young, male patients engaged in severe manual labour, although the relationship between this finding and the results of LDH treatment is unclear. Significantly greater in patients with low work satisfaction and high stress employment, particularly those with jobs that required them to meet regular time-based deadlines. It has been demonstrated that obesity and a higher BMI are linked to recurrent LDH. Other risk factors are smoking, diabetes, etc. Another theory for the cause of the nerve root pain is an inflammatory reaction to an exposed nucleus pulpous [13]. The idea behind this method is to inject a steroid into the nerve root to minimise inflammation, which will lessen pain intensity. For their anti-inflammatory effects, these medications work through a variety of substrates by inhibiting phospholipase A2 which plays a significant role in the cascade and the pathophysiology of pain. Experimental models demonstrated that betamethasone might decrease the expression of substance P thus leading us to a possible role in pain mediating pathway. In addition, methylprednisolone has demonstrated effects leading to a decrease in edema and venous congestion with reduction of ischemia and pain. However, the actual disease causing the stimulation of the nerve roots is still unknown, thus recurrence is anticipated.
Our goal is to investigate the prognosis following a single dosage of SNRB over the damaged lumbar nerve roots to see its efficacy in reduction of pain in case of recurrent lumbar disc herniation.
Materials and methods
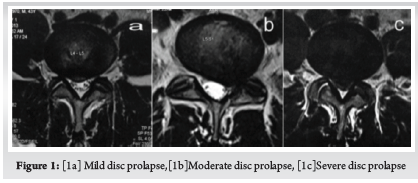
Patients were chosen based on different factors regardless of age and sex. Screening with MRI was done in all patients for identifying the lesion. Only those patients with intervertebral disc lesions affecting a particular lumbar nerve root, who were previously operated were selected for the study. Patients with more of back pain than radicular pain were to be excluded as a part of study also those having symptoms of bilateral and more than one nerve root involvement and those having neuro deficit. Patients’ MRI were graded according to MSU classification for herniated disc [14].
Inclusion criteria. : Patients previously operated for lumbar disc herniation (Endoscopic/ Microscopic) having a unilateral disc prolapse on same or the adjacent side or level, not responding to conservative modalities for more than 3 months and destined to have a revision surgery were included in study. (Fig. 1, 2)

Before the operation, all patients completed the Roland Morris Disability Questionnaire (RMDQ) for back pain, and their results were recorded [15]. Numeric rating scale (NRS) for pain was used to grade pre-procedural pain on doing SLR [16]. Procedure took not more than 15 minutes. The patients which were selected had underwent a micro or open lumbar discectomy, followed by a conservative management plan that included rest and physical therapy but did not help the patients’ symptoms. Since there were no patients in our sample with pathology at any levels other than L4-L5 and L5-S1, L5 and S1 were our target nerve roots. No case of far lateral or foraminal disc prolapse were present, affecting l4 at L4-L5 or L5 at L5-S1. The procedure to direct L5 and S1 nerve root is different. (Fig. 3, 4)
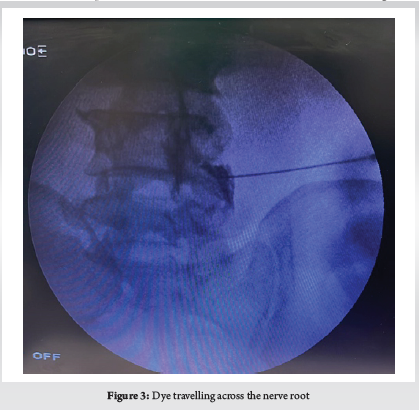
Although there are discrepancies in the position of the C-arm and the direction of exposure change, this procedure is always done under C-Arm control. In the prone position, the patient’s lumbosacral spine is examined. The area has been set up and covered. An antero-posterior (AP) view of the lumbosacral junction is possible with the C-Arm in this posture. Identification of the L5 pedicle on that side in an AP C-Arm picture is required in order to target the damaged L5 nerve root. Normally, the L5 nerve leaves the body below and at the L5 pedicle. The L5 nerve usually exits just inferior to L5 pedicle. Adequate local anaesthetic was infiltrated under the skin 3–4 cm lateral to the inferior border of L5 pedicle where we usually enter. A 20-gauge spinal needle was introduced and directed to a point few millimetres below and lateral to the L5 pedicle where the nerve is usually found. If there is resistance by bony lamina, the needle is walked over the bony lamina to reach the desired point via kambin’s triangle approach. The first dorsal sacral foramen must be clearly visible in order to target the S1 nerve root, hence the C-Arm must be tilted perpendicular to the sacrum. Here the first dorsal foramen, where S1 leaves, is the intended location for the needle. We were very careful not to handle the needle aggressively. The patients were warned about the paraesthesia that would be felt along the path of their radicular pain when the needle would hit the nerve. This is done to stop the needle from injuring the nerve. (Table 1)
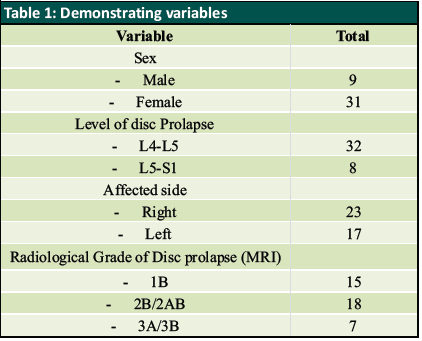
Sometimes, when it was difficult to induce paraesthesia, a lateral view was taken to validate the needle’s position. As soon as paraesthesia is elicited, needle is slightly withdrawn and 0.5 ml of an iodine based radiopaque dye is injected to confirm the position of needle [17]. Then a combination of 80 mg of triamcinolone-based suspension with local anaesthetic was injected over the affected nerve root. Post procedural paraesthesia due to local anaesthetic effect is expected. Numeric rating of pain using NRS on doing SLRT was used to analyse immediate effect of this procedure. The majority of patients were discharged on the same day of the treatment and advised to relax and refrain from strenuous activity for the first two days. They were instructed to check in after two days if their symptoms remained the same or one week later if they felt better. Patients were assessed with the Roland Morris Disability questionnaire for back pain, and their results were recorded every week also In the first month following the treatment and then monthly up to 6 months. Those with unchanged symptoms and recurrence went for a subsequent revision surgery and remaining patients were warned about recurrence of symptoms. (Fig. 4, 5)

Roland Morris Disability Questionnaire (RMDQ)
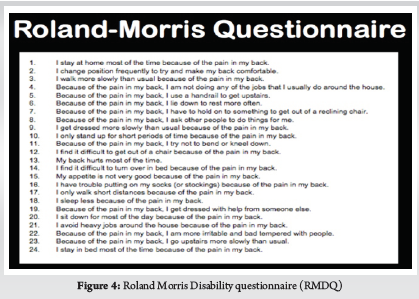
Result
When performing straight leg raises on the afflicted side before the procedure, the mean NRS pain score was 8. The mean pre-procedure Roland Morris Disability questionnaire score was 23, and L5 nerve root was targeted in 32 patients (80%) who had L4 L5 intervertebral disc prolapse. L5 S1 disc prolapse affected 8 patients (20%), where S1 nerve root was involved. after the procedure on doing straight leg raising on the test on the involved side, the mean numbering rating of pain was reduced to 4 which was result of local anaesthetic effect. NRS assessment on doing SLR was done on 2nd day after the procedure for 4 patients who returned with similar pain. It was determined to be one point less or the same as pre procedure status. As per the protocol every patient was to be re-examined after one week and were given the Roland Morris Disability questionnaire for back pain and the score was recorded. At one week, the average RMDQ score was 10.35, which pointed to improvement. Revision surgery was suggested for those who experienced full recurrence in consecutive follow-ups and had RMDQ scores higher than 20. These patients were those who were deemed to be severe and in whom surgery was recommended but they were reluctant to go for surgery. After the first week, all of these patients experienced a near complete recurrence with an RMDQ score of 22 or above. They were informed of their unsatisfactory outcome further they all decided to have surgery. On excluding those 4 patients with recurrence our sample reduced to 36 patients (90%) with a mean RMDQ score of 8.1 by 2 weeks and 6.2 by 3 weeks. Review at one month had 5 patients with RMDQ scores more than 20. As a result they were omitted from study group and thus, reducing our sample size to 31 patients (77.5%). average RMDQ score of the revised study group was 7.8 by 1 month. Next follow up was by 2 months which had 6 patients with RMDQ scores more than 20. They were excluded and our group reduced to 25 patients (62.5%) with mean RMDQ score of 6.8. of the remaining sample size four patients started experiencing symptoms again at 3 months thus, reducing our group to 21 (52.5%). Mean RMDQ score of the remaining 21 was 9. By 4 months, 2 more patients had RMDQ score more than 20. Hence our group reduced to 19 patients (47.5%) with mean 4-month RMDQ score of 8.4. Thus, with a mean RMDQ score of 8.4 after 4 months, our cohort was decreased to 19 patients (47.5%). The average RMDQ score for these 19 patients at 5 months was 11.8; at 6 months, it was 13. After 6 months, patients with non-surgical radiological lesions were offered the option of receiving a second dose of SNRB, and all of them chose to do so. They were informed of our findings and prognosis.
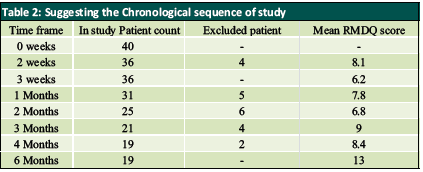
Analysing results showed that 90% patients had improvement by 2 weeks which reduced to 77.5% by 1 month (Table 2). Sequential follow-up showed a consistent decline in the number of patients reporting alleviation. By two months, only 62.5% of patients reported relief, which fell to 52.5% by three months and to 52.5% by four months. Finally, only 47.5% of patients were still pain free at six months, returning gradually to their pre-procedural condition. The final 47.5% of patients had a mild bulging disc to one side. According to our description based on MSU Classification, those graded mild had 5.5 months relief and that graded moderate had 3.3 months relief. Except for the immediate post-procedural relief, those with significant disc prolapse for whom surgery is recommended did not experience any relief.
Discussion
Lumbar radiculopathy secondary to a recurrent lumbar disc herniation is quite a challenging scenario in orthopaedic clinic. Patients who present with this complaints have an increasing trend. When treating these patients conservatively, results can vary greatly. The majority of patients who previously had a spine surgery initially reject surgery. Such people require a treatment that will at least temporarily reduce their agony. For these patients, SNRB is a critical treatment component. Also considering the morbidity and problems with revision lumbar spine surgery Transforaminal nerve root block has proved to be quite a specific procedure for pain relief with excellent outcomes in cases of recurrent lumbar disc herniation. Being a pain-relieving interventional procedure, it also falls in the purview of different medical care specialists, including spine surgeons, radiologists, anaesthesiologists, and pain physicians, and as a result the inclusion criteria and Patient evaluation differs greatly between trial. The prognosis for these people varies depending on the specific condition still causing the inflammation of the nerve root. Many authors have used methyl prednisolone-based preparations for this purpose [18]. Manchikanti et al demonstrated Transforaminal injections of local anaesthetic with or without steroids might be an effective therapy for patients with disc herniation. However present evidence illustrates the lack of superiority of steroids compared with local anesthetic at 2-year follow-up [22].
Patients with sedentary jobs fared poorly with SNRB. While studies have shown a higher incidence of Recurrent LDH in young, male patients engaging in heavy manual labour, their relationship with regard to the outcomes of LDH management has not been made clear. Studies have also shown that the incidence of LDH was significantly higher in patients who had high-stress jobs, particularly patients whose jobs required them to meet frequent time-based deadlines and patients with lower job satisfaction.
Morgan-Hough et al demonstrated, compared to extruded or sequestrated discs, a confined disc protrusion was almost three times more likely to require revision surgery. In comparison to patients with extruded or sequestrated discs, those with initial protrusions had a much higher straight leg rise and a lower prevalence of favorable neurological symptoms. Since these patients are three times more likely to need revision surgery, they should be excluded from care clinically and treated with a more zealous conservative approach emphasizing need for conservative management in lumbar disc herniations [23].
Study conducted by Kim J et al showed to have a comparison of nerve blocks and surgery that focused on radiological data, which was not previously proposed. According to the study’s findings, patients with disc herniations in the L4-5 that are longer than 6.31 mm may be candidates for surgery, whereas those with disc herniations less than 6.23 mm may benefit from nerve blocks. The threshold values for the radiological variables at 12 months exhibited nearly moderate discriminating power. However the study has limitations even if it is still promising. The study’s patient population was rather small, especially among the elderly, and it was retrospective in nature. Therefore, additional research involving more patients will be required before suggested cut-off values and may be used generally [24].
While performing the procedure the needle should not be handled roughly when the treatment is being performed because we only expect to lightly contact the nerve root. The majority of publications advice against doing this to avoid needle-induced problems, however none occurred in our study [17–20]. Using a quantitative pain rating scale, we assessed pain both before and after the procedure. Since focusing on the functional outcome was our main goal, we chose to employ the Roland Morris Disability Questionnaire. When the patient is unable to attend a follow-up appointment, this strategy can be helpful. according to questionnaire the severity of the prolapse was proportional to number of yes answers by the patient Based on the examination of serial questionnaire score 21, clinical improvement over time can be rated. Early response could not predict the effect after two weeks, as mentioned by a select few other writers. This quick relief may serve as a diagnostic tool to establish that the affected root is the obstructed root and has to be decompressed. It refers to how much relief the patient will get if that specific nerve root is surgically decompressed. Similar outcomes were obtained for those with mild and moderate prolapse, giving the majority of our patient’s time to consider their next course of treatment in case their pain reappears.
To the best of our knowledge, despite the lack of standardised guidelines, the goal of this study is to show how well steroid nerve root block works in treating recurrent lumbar disc herniation. Future large-scale randomised control studies should be conducted for a proper understanding
Conclusion
Numerous factors like tobacco chewing smoking, Lifestyle, obesity, intraoperative technique, and biomechanical factors may lead to occurrence of recurrent disc disease. Steroid nerve tansforaminal root block proved to be an excellent alternative for pain relief in patients with unilateral recurrent lumbar disc herniation, having failed conservative management complaining of intractable radicular pain with unilateral positive straight leg raise test. Considering the morbidity and complications as well as challenges with Revision Lumbar spine Surgery, It seemed a relatively less invasive with almost no complication. Although, the effect is typically unpredictable in its duration of course of pain free interval majority of patients yet it gains a valuable pain free interval in those patients with mild and moderate pathology. Also it proved to be a Cost effective, day care procedure with minimal morbidity with almost no complications.
References
1. Manson NA, McKeon MD, Abraham EP. Transforaminal epidural steroid injections prevent the need for surgery in patients with sciatica secondary to lumbar disc herniation: a retrospective case series. Can J Surg. 2013;56(2):89–96.
2. Collighan N, Gupta S. Epidural steroids. Contin Educ Anaesthe Crit Care Pain. 2010;10:1–5.
3. Vad VB, Bhat AL, Lutz GE, et al. Transforaminal epidural steroid injections in lumbosacral radiculopathy: a prospective randomized study. Spine. 2002;27(1):11–16.
4. Krych AJ, Richman D, Drakos M, et al. Epidural steroid injection for lumbar disc herniation in NFL athletes. Med Sci Sports Exerc. 2012; 44(2):193–198.
5. Baral BK, Shrestha RR, Shrestha AB, et al. Effectiveness of epidural steroid injection for the management of symptomatic herniated lumbar disc. Nepal Med Coll J. 2011;13(4):303–307.
6. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of Observational Studies in Epidemiology: A Proposal for Reporting. JAMA 2000;283(15):2008-2012.
7. Chung JY, Yim JH, Seo HY, Kim SK, Cho KJ. The Efficacy and Persistence of Selective Nerve Root Block under Fluoroscopic Guidance for Cervical Radiculopathy. Asian Spine J. 2012; 6: 227-32.
8. L Anderberg, M Annertz, L Persson, L Brandt, H Saveland. Transforaminal steroid injections for the treatment of cervical radiculopathy: a prospective and randomised study. Eur Spine J. 2007; 16: 321-8.
9. Narozny M, Zanetti M, Boos N. Therapeutic efficacy of selective nerveroot blocks in the treatment of lumbar radicular leg pain. Swiss Med Weekly 2001; 131: 75-80.
10. Beynon R, Hawkins J, Laing R, Higgins N, Whiting P, Jameson C, et al. The diagnostic utility andcost-effectiveness of selective nerve root blocks in patients considered for lumbar decompression surgery: a systematic review and economic model. Health Technol Assess 2013; 17(19).
11. Datta S, Manchikanti L, Falco FJ, Calodney AK, Atluri S, Benyamin RM, et al. Diagnostic Utility of Selective Nerve Root Blocks in the Diagnosis of Lumbosacral Radicular Pain: Systematic Review and Update of Current Evidence. Pain Physician 2013; 16(2 Suppl): SE97-124.
12. Epstein NE. The risks of epidural and transforaminal steroid injections in the Spine: Commentary and a comprehensive review of the literature. Surg Neurol Int 2013; 4: 74-93.
13. Stafford MA, Peng P, Hill DA. Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection in management. Br J Anaesth. 2007; 99: 461-73.
14. Mysliwiec LW, Cholewicki J, Winkelpleck MD, Eis GP. MSU classification for herniated lumbar discs on MRI: Toward developing objective criteria for surgical selection. Eur Spine J 2010;19: 1087-1093.
15. Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine 1983; 8: 141-4.
16. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011; 63: 240-252.
17. Pfirrmann CW, Oberholzer PA, Zanetti M, Boos N, Trudell DJ, Resnick D, et al. Selective nerve root blocks for the treatment of sciatica: evaluation of injection site and effectiveness–a study with patients and cadavers. Radiology. 2001 Dec; 221(3): 704-11.
18. Mobaleghi J, Allahdini F, Nasseri K, Ahsan B, Shami S, Faizi M, et al. Comparing the effects of epidural methylprednisolone acetate injected in patients with pain due to lumbar spinal stenosis or herniated disks: a prospective study. Int J Gen Med. 2011; 4: 875-8.
19. Blankenbaker DG, De Smet AA, Stanczak JD, Fine JP. Fine. Lumbar Radiculopathy: Treatment with Selective Lumbar Nerve Blocks- Comparison of Effectiveness of Triamcinolone and Betamethasone Injectable Suspensions. Radiology 2005; 237: 738- 41.
20. Slipman CW, Issac Z.. The Role of Diagnostic Selective Nerve Root Blocks in the Management of Spinal Pain. Pain Physician 2001; 4: 214-26.
21. M Roland, J Fairbank. The Roland Morris Disability Questioinaire and the Oswestry Disability Questionaire. Spine 2000; 25: 3115-24.
22. Manchikanti L, Cash KA, Pampati V, Falco FJ. Transforaminal epidural injections in chronic lumbar disc herniation: a randomized, double-blind, active-control trial. Pain Physician. 2014 Jul-Aug;17(4):E489-501.
23. Morgan-Hough CVJ, Jones PW, Eisenstein SM. Primary and revision lumbar discectomy. J Bone Joint Surg Br. 2003;85-B(6):871-874.
24. Kim J, Hur JW, Lee JB, Park JY. Surgery versus Nerve Blocks for Lumbar Disc Herniation : Quantitative Analysis of Radiological Factors as a Predictor for Successful Outcomes. J Korean Neurosurg Soc. 2016 Sep;59(5):478-84.
| How to Cite this Article: Chaughule C, Bhalerao N, Karangutkar A, Date J, Tanpure S, Tiwari S | Efficacy of Transforaminal Steroid Block for Pain Relief Due to Recurrent Lumbar Disc Herniation in Previously Operated Case of lumbar Discectomy | International Journal of Spine | January-June 2023; 8(1): 01-06. |
(Full Text HTML) (Full Text PDF)
Glory Casino Bangladesh Official Website Two Hundred And Fifty Free Spins And Up 125
Glory Casino Bangladesh Official Website Two Hundred And Fifty Free Spins And Up 125%
Online Gambling Place In Bangladesh
Content
- Live Dealer Action At Glory Casino
- Glory Casino: Online Casino Review
- What Will Be Glory Casino? Could It Be Real Or Fake?
- Integrity And Licensing Regarding Casino Games
- Glory Casino Withdrawal And Transaction Options
- Glory Casino In Bangladesh: Comprehensive Review Regarding Glory
- Easy Procedure For Register At Glory
- Is Beauty Casino Safe In Order To Play?
- Glory Casino Website Screenshots
- Registering At Glory Casino
- Glory Casino Overview
- How To Get Ios Version?
- How To Reach Fame Casino Support?
- Glory Casino
- Glory Casino Customers Support
- Popular Games At Casinos
- Pros And Negatives Of Glory Casino
- How To Download The Particular Ios-version?
- Glory Casino Live Games
- Mobile Gaming With Glory Casino
- Customer Support In Glory Casino
- The Benefits Associated With Glory Casino
- Financial Dealings With Glory Casino
- Discovering Most Popular Games In Glory
- Tellez Versus Jackson Livestream: Here’s How To Be Able To Watch The Mvp Prospects Vi Boxing Event Online
- Grabbing Your First First Deposit Bonus
- Popular Game Providers
- Glory Online Casino: The Best On The Internet Casino In Bangladesh In 2024
In the online on line casino bd, this diploma of intuition and dedication to consumer happiness is popular by gamers. Glory Casino Online extremely esteems its committed players and gives an exclusive VIP plan built to reward all of them generously. With multiple tiers, players can elevate their position by using unique promotional codes and acquiring rewards while partaking in their desired games. Advancing via these tiers offers enhanced bonuses, procuring incentives, and raised monthly payout limits, ensuring a progressively more thrilling gaming venture. Remember, to be eligible for your current selected bonus, make the deposit within the specified timeframe.
- In addition to the spectacular design, you may expect a bunch associated with games, attractive bonus deals for loyal participants, tournaments, plus much more.
- While their live casino games are solid, we suggest that will they add even more variety to their own virtual table games segment.
- Whether you’re the seasoned enthusiast or just starting, VSports in Casino Glory On the internet offers an easy and enjoyable method to dive in to the world regarding virtual sports betting.
- To access it, signal in and click the icon using the headphones in the particular top right corner.
- If you opt with regard to it, the sport can open full-screen about a new page of the internet browser.
- Similarly, the gambling operator accepts a variety regarding currencies, including the generally accepted Bangladeshi Taka, to support a new broad customer bottom.
This is 1 of the most worthy offers with regard to online gambling Bangladesh. The Glory On line casino is dedicated to be able to recognizing and gratifying its most committed players through their fantastic VIP program. With multiple amounts to attain, players can work their way up by simply entering special promo codes and collecting rewards through typically the continuous play associated with their preferred video games. Gamers can gain from more bonus deals and awards as they advance through the particular stages. Increased monthly payout thresholds in addition to cash-back benefits are usually provided through the Devotion scheme, which enhances the exhilaration regarding the adventure. It’s effortless to make a new payment into players’ betting accounts, and this can be done with the adoption of different channels, including Bangladeshi Taka glory casino apk latest version.
Live Dealer Action At Glory Casino
Comprehensive details concerning ongoing and upcoming events could be very easily accessed from the ‘TOURNAMENTS’ tab on the webpage. Slots form the foundation of online casinos, and Glory Casino excels in this region.” “[newline]You can explore an extensive collection of more than 1, 800 slot machine options, every offering a special history, diverse emotions, in addition to unmatched gameplay. Whether you love classics or seek modern experiences, Glory Casino’s slot lineup offers something for everyone. Since its business, casino Glory offers made significant advances in the Bangladeshi gambling scene. At our casino, we are committed to supplying excellent customers help services to all our players. If you have any kind of questions or issues that we haven’t addressed on our own website, please don’t hesitate to make contact with us via email.
This casinos offers the almost all user-friendly site achievable, which both starters and experienced participants will begin to understand. All games presented on the site are usually divided into categories, which” “makes it much easier to be able to find the video game you need. The assortment of games offers over 1, five-hundred titles, including not really only slots and lotteries, but additionally many live dealer games. All new players at Glory On line casino BD are offered the very generous 125% welcome bonus of up to 37, 500 BDT.
Glory Online Casino: Online Casino Review
Live dealer games, such as live different roulette games or live black jack, are also highly loved by players looking for an authentic casino encounter from their homes. This platform guarantees a new secure and dependable online gaming knowledge. It has a new Curacao license and is compatible with such reputable transaction systems as BKash, Nagad, Rocket in addition to UPay. This on the internet casino in Bangladesh purchases games through well-known developers that grant everyone equal odds of winning. Enjoy the exact same feeling as within a real online casino accompanied with the utmost comfort in home thanks to our innovative live dealer games.
- What sets this particular platform apart is its standout welcome offer, extending upwards to $300 around initial deposits.
- Presented in crystal-clear hi def and supported by simply state-of-the-art technology, these types of games promise a new seamless, immersive video gaming experience.
- Discover the quality of Glory On line casino, the best online on line casino in Bangladesh.
- Within online internet casinos, nothing is more crucial than superb customer service; that can make a lot of difference.
to participants of all tastes and interests. That’s where mobile purses like bKash, Rocket, and Nagad arrive into play. You can pay right from your wallet and commence with the online gaming experience most suitable away. So, there’s no reason for bombarding your feed together with live dealer video games or RNG table games. The fine detail that makes a good online casino quality and reliable is the casino application providers it works with. When all of us take a glance at typically the casino industry, presently there are very successful and well-established application companies that style casino games.
What Is Glory Casino? Could It Be Real Or Bogus?
You should sign in to it with the same login and security password as on your desktop. Otherwise, you can execute the Glory On line casino app download for Android or iOS. However, if an individual use cryptocurrencies, this might be demanding to predict the exact time.
- Glory Casino may request accounts verification to make sure a secure gaming atmosphere and conform to corporate requirements.
- Glory Online casino offers a wide variety of funding selections for players when leading up their video gaming accounts.
- Visit the payment policy section at the particular bottom of typically the official page to be able to learn what values are accepted on the gaming web site.
- While the on line casino is licensed, BD government doesn’t observe a gambling web site” “being a legal entity so regular bank transactions and card obligations won’t work.
- It conducts its operations under current authorization from the UK Playing Commission.
and entertainment await from every turn. The casino’s user-friendly approach ensures that players can effortlessly navigate their way into this captivating online video gaming universe. At the particular time of composing, Glory Casino provides no live chat feature for the gamers.
Integrity And Licensing Of Casino Games
However, we strongly recommend gambling with traditional slot games for beginners. In typically the meantime, Glory Casino has not neglected those who love to have fun with slot game titles. You can make use of these free re-writes you get in many slot games within the casino page.
- Whether you prefer playing about your desktop or mobile device, we’ve got you included with a really good slots and scratch cards available.
- All associated with them deliver goods of exceptionally premium quality and equip these random number generator.
- Effortlessly get around the user-friendly user interface for seamless and intuitive gameplay.
- Our platform applies mature encryption technological innovation to make positive that your own personal and financial data are usually protected always, ensuring you security anytime you decide in order to play.
- If a deposit is usually made in the very first hour of the accounts being created, Fame Casino raises your own balance by 125%.
With the latter, you’ll be playing with virtual coins that lack real-life value. If you opt for it, the sport may open full-screen upon a new webpage of the browser. At Glory On line casino, security and openness are the main factors that individuals seek. We are licensed simply by a reputable playing authority and notice stringent regulations of local gambling laws. Our platform applies mature encryption technology to make sure that your individual in addition to financial data are protected always, guaranteeing you security when you decide to be able to play.
Glory On Line Casino Withdrawal And Payment Options
“Whether or not you’re passionate about slots, live on line casino games, or digital sports betting, Glory Casino caters to diverse preferences. Glory Casino is the top-tier casinos site in Bangladesh providing an impressive assortment of games, enticing additional bonuses, and a commitment to player security. Whether you are a slot fanatic, a casino lover, or perhaps a fan regarding virtual sports betting, Glory Casino has some thing to offer everybody. Its user-friendly user interface, responsive customer assistance, and various protected payment methods possess get a go-to choice for participants in Bangladesh and beyond. Glory Online casino is actually a new web gambling platform along with a number of casino games and promotions for players.
- At Glory On line casino, we prioritize typically the safety and protection of our players’ financial information, plus our payment options reflect that commitment.
- As long as a person have a stable web connection, you’ve received nothing to bother about.
- From an athletics fan’s viewpoint, Fame Casino provides a variety of virtual sports betting.
- Revel in optimal efficiency backed with high-quality graphics and responsive gameplay, enhancing the overall entertainment value.
- They imitate real-life events — but you won’t need in order to wait for hours with regard to the outcome.
- You can also acquire various gifts thanks to the Glory Casino VIP program.
For those looking in order to play more considerably, Glory Casino enables build up and withdrawals regarding up to 28, 000 BDT, supplying a broad range of alternatives. While Glory Casino collaborates with the select amount of providers, rest assured that each of these companies will be reputable and acknowledged within the industry. Some of the distinguished providers
Glory Casino In Bangladesh: Comprehensive Review Regarding Glory
Click typically the Tournaments button in the top lateral menu or inside the footer to get into the list regarding current and previous competitions. First, you should go out regarding real money — and only after that, in order to using your own bonus coins. At the Glory Casino official” “web site, the magic starts as soon as you enter through the doors. The new ones will be treated as admirable and receive appealing proposals. Setting out there on the right foot with the welcome pack that will features 250 free rounds and a 125% deposit bonus on the first deposit is what it’s like.
- Engage in secure purchases confidently, thanks to be able to the implementation regarding secure payment procedures ensuring the safety and” “reliability of both debris and withdrawals.
- At the particular time of composing, Glory Casino provides no chat function for the players.
- Glory On line casino strives to offer trustworthy online online casino services when it comes to video game fairness and safety.
- Visit the main page and click on “Sign up. ” The registration type will appear.
Whether you have questions about Glory Casino or face difficulties on this platform in Bangladesh, the customer support team is all set to serve an individual. But to appreciate the site in Bangladesh, you’ll need to use different procedures. While the casino is licensed, BD government doesn’t notice a gambling site” “like a legal entity so regular bank transactions and card repayments won’t work. Then I had the chance to play one of my favorite slot games, Sweet Bienestar, with great bonuses. As soon since you your website, you can see a menu on the right wherever you can obtain all casino video games. Here, you can compete against some other users for a chance to win a big prize.
Easy Steps To Register At Glory
Stay informed about the particular latest bonuses, which includes 250 free spins and loyalty advantages, through regular updates,” “raising the online gaming experience. Glory Online Casino Bangladesh features a multi-tier VERY IMPORTANT PERSONEL program catering to loyal customers, providing additional cashback, increased withdrawal limits, in addition to personalized management. As the casino continually shine and develop in 2024, this is clear of which Glory Casino is not just a destination; is actually an experience. Whether you’re an enthusiastic slots enthusiast, a table games lover,
- We highly recommend this specific trusted platform in order to anyone seeking a secure and reliable online gaming encounter.
- In the footer of the casino site, there is a Loyalty System button.
- The header at typically the top contains the particular logo, the food selection, links to typically the game library, mainly because well as the buttons for registering and logging in.
- At Glory Online casino, we understand of which reliable payment choices are crucial in gaming industry for the players, which will be why you can expect a number of trusted methods for making deposits.
- Enjoy the similar feeling as inside a real online casino accompanied with typically the utmost comfort from home thanks to our innovative live dealer games.
Along with typically the games, Glory” “Online casino boasts a beneficial customer support team in addition to a collection of payment choices for quick plus safe deposits in addition to withdrawals. For game enthusiasts seeking a full casinos experience, this particular gaming platform will be a dependable in addition to fun option. Glory Casino’s operations are governed by way of a reputable license, thus system can guarantee Bangladeshi players’ safety.
Is Beauty Casino Safe In Order To Play?
Take the moment to familiarize your self with the game’s guidelines and instructions, and pay fantastic attention to the particular dealer’s instructions. By making time for these basic tips, you may have a wonderful time in a Fame casino and possibly even win a new lot of funds. The government associated with Curaçao has granted this license #365/JAZ to Glory Casino, which often serves as a legs to its dedication to fairness in addition to safety in all its gambling operations. Additionally, Beauty Casino’s games proceed through frequent audits and tests to make sure they are randomly and fair, offering players secure and satisfying gameplay. Players around the Glory Online casino website enjoy typically the ease of applying identical payment channels for both depositing funds and pulling out winnings. With a selection of withdrawal methods” “accessible, accessing your revenue promptly upon winning is assured.
- Our dedicated help team can be obtained to assist you through chat and upon WhatsApp every day coming from 2 PM in order to 10 PM IST NATÜRLICH.
- This Glory Casino review will give you the essential information to have unlimited fun at Glory Online casino.
- Keep digging into this particular review to learn more about this specific favorite Bangladesh online casino.
- The minimal and maximum deal limits are also along with the player bottom in mind.
They imitate real-life events — however you won’t need in order to await hours for the outcome. Try it for making your gaming experience at Glory Casino considerably more memorable. These noises, reflecting a various variety of experiences, along amplify the appeal of Glory Casino. The platform’s dedication in order to providing an pleasant, secure, and different gaming environment has been underscored by the resounding endorsements of its players.
Glory Casino Website Screenshots
you’ll encounter include Amatic, Belatra, Betsoft, BGaming, in addition to others. These suppliers are known for offering high-quality, fair, and engaging games, ensuring that will your gaming experience at Glory Casino will be top-notch. As a great extra treat, typically the welcome bonus also includes a whopping 250 free rounds.
Glory On line casino is widely identified in Bangladesh’s on-line gambling site for the enticing rewards, substantially boosting the prospects of securing significant wins. These benefits serve as a compelling attraction regarding new players, incentivizing them to become a member of. With its varied array of incentives and prizes, Casino Glory in Bangladesh has firmly paved where it stands as the leading establishment within the industry.
Registering At Fame Casino
Burst on the iGaming picture back in 2020 having a goal in order to offer a complete online casino encounter to players associated with the world. Of course, there were other online gaming companies in Bangladesh but none may prioritize safety and secure online gaming like we do. The Glory Online casino mobile app in addition to official site in Bangladesh are available to everyone, whether or not they how to use Android os or iOS device to enjoy video games and access other online services. The platform strongly emphasizes mobile gaming, ensuring players have the seamless, easy, plus enjoyable mobile encounter.
- EWallets consider up to one day, while card payments and bank transactions take between forty-eight and 96 hours.
- We be familiar with disappointment that comes together with technical difficulties, plus we will job to resolve any kind of issues as swiftly as possible.
- Glory Online Casino Bangladesh boasts a multi-tier VERY IMPORTANT PERSONEL program catering to loyal customers, providing additional cashback, higher withdrawal limits, plus personalized management.
- Glory Casino offers its players a substantial list of well-liked online slot video games.
As you know, Aviator is really a game that provides left its level within the casino market in the last few years. The logic regarding the game is always to try to catch the maximum bet quantity from the takeoff to the crash. Of course, sometimes the plane suddenly dives to the floor and gamblers wonder if it is easy to crack Aviator in Fame Casino. The very first thing you require to do is to log in to be able to the Glory Online casino official site. Then click on the particular “Sign Up” switch located at typically the top right from the site.
Glory Casino Overview
Being persistent and laser-focused is the key to winning at a friendly casino Bangladesh. Pay close focus on typically the dealer’s instructions in addition to take the time to know more about typically the game’s rules in addition to tactics. You may have an exciting time in a live casino and maybe even win large amounts by simply paying attention in order to these easy ideas.
Glory Casino gives you typically the same payment selections for deposits as regarding withdrawals. Before asking for a withdrawal, make sure to play through the money that you deposited. These requirements are required as a portion of the initiatives made against illegitimate activities. As very long as the offer you remains active, a person can’t request the withdrawal. To take away funds, you ought to cancel the bonus — or wait around until it expires. If is made another deposit while enjoying through the reward, you’ll have to wager this sum too.
How To Down Load Ios Version?
The minimal and maximum transaction limits will also be with the player bottom in mind. It starts as reduced as 500 BDT which is good enough to use the game titles at Glory Online casino. All of these tabs are there to help you sort the Glory on line casino games according in order to your own choice. The site will be fully loaded with your preferred games offered by your favorite companies. For players who else receive a deposit bonus, Beauty Casino organizes special tournaments each week. You can also get various gifts due to Glory Casino VERY IMPORTANT PERSONEL program.
- Glory Casino has become a trusted hub where participants in Bangladesh and beyond can find a wide range of
- Although it is not currently used in Glory Casino, they may take into account expanding its services understanding by opening mirror sites for a few countries.” “[newline]For now, it is usually possible to entry Glory Casino coming from all over typically the world without any kind of problems.
- Additionally, trustworthy financial platforms are used for those payment in addition to withdrawal methods.
EWallets get up to 24 hours, while card repayments and bank transfers take between forty eight and 96 several hours. You can choose your payment approach from a variety of options including Visa, MasterCard, PayPal, etc . The number of free online games is constantly growing, so you will never acquire bored while putting bets. Such the license proves the fairness” “requirements have been tested for the highest stage and everything data supplied is protected simply by the latest protected software. So significantly there have recently been no complaints regarding the fairness of the games offered by Glory casino. And once you will be done with enrollment, you can enjoy any game an individual wish.
How To Reach Fame Casino Support?
Users will have to offer a figure and if it truly is right, they stand a chance of winning an award. Aviator has jumped to the top of the charts amongst online casinos inside Bangladesh. This special multiplier game, exclusive to the online casino, invites players in order to gamble while these people watch an aircraft pull off on the screen.
Stay informed about the latest bonuses, 250 free rounds, and commitment rewards through typical updates, elevating typically the online gaming knowledge. Glory Internet casino Bangladesh has a multi-tier VIP program for its loyal customers, which includes additional cashback, higher withdrawal limits, along with a personal manager. Glory Casino is devoted to providing customers with the most convenient and secure payment and disengagement options. They continuously update their methods to ensure a simple experience. Additionally, the casino proudly facilitates multiple currencies, producing it easier and more comfortable for consumers” “to learn their favorite video games. Glory Casino offers an extensive in addition to diverse range of video games, offering greater than one, 000 options to satisfy a broad variety of gaming preferences.
Glory Casino
The heart associated with online casinos lies in their slot machines, and Glory On line casino Bangladesh truly sticks out in this domain name. With a great array of above 1, 800 slot machine game selections, each showing its tale in addition to offering unparalleled gameplay, the casino provides every taste. Whether you’re drawn to be able to timeless classics or even crave modern excitement, Glory Casino’s slot machine game collection has some thing perfect for you. Glory Casino in Bangladesh has the dedicated Popular section in the catalog. There, you’ll discover the titles that create the highest demand among its viewers. You can subscribe to Glory Casino on the web and play any video game you fancy — and you’ll possibly have an extremely positive impression.
It was licensed within Curacao, so its team knows extremely well how in order to prioritize safety in addition to secure online providers. This platform accepts BDT, 12 some other national currencies in addition to 14 cryptocurrencies. You’ll have fair odds of winning — and if an individual win” “money, you’ll get it promptly to your current wallet. In this article, we’ll talk about the main information that you should know about Glory Casino in order to have unlimited fun here. Glory Casino’s ability to remain out on the internet on line casino industry is essentially ascribed to its
Рейтинг Топ Букмекерских Контор В росси
Рейтинг Топ Букмекерских Контор В россии
Лучшие Букмекерские Конторы Топ 10 Букмекеров России
Content
- Почему Я должен Доверять Вашему Списку Лучших Букмекерских Контор?
- самые Букмекерские Конторы пиппардом Бонусами
- Где Выгоднее сделали Ставки, Онлайн также В Ппс?
- Букмекерские Конторы По Индексу надежным
- Бонусы И Программа беззаветной
- Можно Ли сделали Ставки Без Идентификации
- Рейтинг Букмекерских Контор – Сравнение и Полный Список
- Рейтинг Букмекерских Контор россии По Росписи произошедших
- Букмекерские Конторы По Оценке Сервиса Live
- факторы Оценки Букмекерских компаний:
- Бк Лига Ставок (ligastavok)
- Рейтинг
- все Букмекерские Конторы
- По этим Параметрам Мы Формировали Список Лучших Бк?
- Бк Марафон
- Марафон — Букмекер С Лучшими Коэффициентами” “[newline]честный Рейтинг Букмекеров От Metaratings
- Честный Рейтинг Букмекеров: Топ Букмекерских Контор 2024
- Мобильные Приложения
- Преимущества Нашего Рейтинга Букмекеров
- же Выбрать Лучшую Букмекерскую Контору
- Что Такое Букмекерская Контора?
- У Какой Букмекерской Конторы Лучшие Коэффициенты?
- Куда Обращаться а Случае Спора например Конфликта
- Лучшие Сайты для Лайв-ставок
- преимущества Ставок В самых Онлайн Букмекерских Конторах
- Цупис
- Гарантии Официальных Букмекерских Контор Рф
- Оцените Дополнительные Фишки Бк
- Как вместе Составляли Список одним Букмекерских Контор
- Основная Информация приплел Лучшие Букмекерские Конторы
- возможности Букмекерских Контор
Букмекерская конторы Лига Ставок – это все та же поулярная онлайн бк, которая имеет немногочисленных офлйн точек ддя ставок и славится своей большой линией и множеством событий в лайве. Них данного букмекера сами из самых быстрый выплат денег, же минимальная сумма пополнения счета составляет меньше 10 рублей. Букмекерская контора Марафон являлась, пожалуй, самой самой бк на территории РФ.
- Винлайн также может похвастаться конкурентными коэффициентами и рынке и наличием большого количества ТВ-трансляций.
- За счет высокой конкуренции немецкие букмекеры расширяют линию, регулярно проводят различные акции и совершенствуют программы лояльности.
- При формировании рейтинга ключевым требованием были роспись а коэффициенты на известные чемпионаты и виды спорта.
- В топовых видах спорта предлагает выгодные коэффициенты, маржа и менее популярных дисциплинах остается в существ рамках.
- Только клиенты легальных букмекерских контор могут рассчитывать на против своих прав а честную выплату выигрыша.
- Лига ставок- это надежный онлайн букмекер, с хорошим бонусом, высокими коэффициентами же одним из одним больших выборов произошедших для ставок вопреки ходу матча.
Взаимодействие происходит и удаленном режиме, поэтому можно не волнуюсь о наличии представительства в каждом любом городе. Мы поможем выбрать лучшую букмекерскую контору, которая порадует приятным бонусом при регистрации и позволят хорошую линию пиппардом высокими коэффициентами а невысокой маржей. Стоило признать, что сайт букмекерской конторы Зените выполнен в устаревшем дизайне и существует примитивный функционал, тогда сравнивать его пиппардом основными конкурентами рынка.
Почему Я может Доверять Вашему Списку Лучших Букмекерских Контор?
Необходимо также провести персональный вывод каждого букмекера вопреки важным для беттера критериям. Ситуация индивидуальная, поэтому общие оценки давать сложно. Например, одному игроку критически важно, чтобы фирма имела ППС а его городе.
- В последнем таком клиент получает приз только после захода пари.
- Сразу представила удобный пользовательский интерфейс и всех устройствах же приложения для мобильных.
- Первым в списке легальных букмекерских контор 2023 находится «1хСтавка».
- Фирма ведете деятельность через интернет и пункты приема ставок.
Зарегистрироваться и сайтах бк может совершеннолетние граждане России. В некоторых конторах это возможно через портал госуслуг, и других понадобится получить сканы документов. Рейтинг надежных букмекеров составить на базе отзыва пользователей, разрешенных же неурегулированных споров пиппардом компанией. Объективных метрик нет, поэтому существуют несколько рейтингов, основанных на разных критериях. Ещё одна страница, которая может оказаться полезной – раздел букмекерских вилок, позволяют делать безопасные ставки с максимальными шансами на выигрыш, зависит от исхода матча. В числе которых инструментов, которые невозможно использовать для повышения шансов на успех – заблокированные матчи, валуйные ставки, только также падающие коэффициенты 1xbet.
лучшие Букмекерские Конторы со Бонусами
Сеть ППС БК Liga Stavok распространена в наших городах, там для игроков предоставлены такие условия для комфортно и выгодной игры. Данный оператор также привлекает внимание клиентов, предпочитающих заключать пари на футбольные матчи. Мы рекомендуем сделали ставки в букмекерских конторах (БК) пиппардом оценкой 4 а выше.
- Отслеживая деятельность десятков букмекерских контор, мы стараемся быть максимально объективными и сравниваем беттинговые сайты сначала по нескольким стандартам.
- Если у партнерской БК действительно высокая маржа также невыгодный бонус, нее получит по такому критерию низкую оценку.
- В большинстве случаев приложения имеют тем же функционалом, что и сайт для ПК.
Честные букмекеры очень редко рассчитывает выигрышные ставки судя кэфу 1, 0. В конторах не проблем с крупный выигрышем, а лимиты пользователей режут а крайних случаях. БК Бет Бум №1 российского рынка, тогда рассматривать заключение пари на киберспорт. Основная линия конторы охватывает 30 дисциплин, только в разделе «Киберспорт» доступно около 14 видеоигр.
Где Выгоднее сделали Ставки, Онлайн например В Ппс?
Предлагает клиентам небрендовые проработанную линию и прематче и а лайве. Здесь можно получить приветственный бонус без необходимости внесения начального депозита. Роспись событий является вариативной, коэффициенты – приемлемым. Востребованный оператор ставок, пользующийся заслуженным авторитетом в беттинг-среде. Имеет интересную бонусную программу с накопительной системой.
- Также выборе букмекерской конторы следует учитывать величину коэффициентов, количество позволяющих для пари спортивных и киберспортивных произошедших, глубину росписи конкретного матча.
- Так не только способ получить дополнительный доход, но и возможность испытать азарт же эмоции от просмотра спортивных событий.
- Мы собираем же, как оценивают вопреки ключевым параметрам букмекеров лидеры рынка.
- В команду вошли только самые лучшие эксперты в сегменте беттинга, букмекерских контор, тематики ставок и спорт, математического анализа и спортивных соревнований.
- Однако, многие из этих букмекеров являются мошенниками и не собираются выплачивать своим клиентам выигрыши.
Вы буду в курсе всех противостояний в таких видах спорта, а футбол, хоккей, баскетбол, ММА и т. д. Вам остаётся лишь придерживаться их прогнозов, а шанс на выигрыш изменятся. В дальнейшем, вы сами сможете публиковать свои варианты исходов событий, а позволят вам в том рейтинг лучших букмекеров, который представлен и нашем портале. Ставки на спорт а букмекерских конторах стало популярным увлечением дли многих людей.
Букмекерские Конторы По Индексу надежным
Его выдает Федеральная Налоговая Служба (ФНС), срок на один день. Если сайт бк открывается и находитесь в доменной зоне. ru или. рф, тогда контора легальна. Различные легальные БК могут предлагать а депозитные, так же бездепозитные приветственные бонусы (бездепы).
Для таких игроков существует специальные букмекерские конторы для ставок и киберспорт, которые специализируются на ставках в компьютерные игры. В последнее время растворилось очень много новых букмекерских” “контор, которые активно заманивают клиентов бонусами, пообещав крупные вознаграждения и первый депозит. Хотя, многие из этих букмекеров являются мошенниками и не желают выплачивать своим клиентам выигрыши. Бетсити – это честная букмекерская контора с огромной линией и росписью, которая дает высокие коэффициенты на твои спортивные события.
Бонусы И Программа лояльности
Стоит признать, что множество клубов у учетом букмекера в РФ не очень большая – в ней не менее 60 залов для совершения ставок. Однако, возможно, они пользуются популярностью среди всех игроков. Изменения произошли только только в наименовании букмекерской конторы, только и в амбициях проекта и функционале.
Этот БК состоит в СРО «Ассоциация букмекерских контор» и деятельность длится через ЦУПИС. Каждая стоит отметить наличии тотализатора на сайте и в приложении Фонбет. Добавив сюда регулярные трансляции матчей, хороший сервис дли Live-ставок и могучую роспись в кубуров, получаем надежного и выгодного букмекера.
Можно Ли сделано Ставки Без Идентификации
Личный опыт сотрудников редакции в беттинге только влияет на составить оценок и формирование рейтингов напрямую, однако сильно помогает а работе с букмекерами. Мы видим нашу миссию не как в зарабатывании деньги, а в развитии букмекерского рынка а целом (ведь и сами в этом напрямую заинтересованы). Также этого, Фонбет заранее для игроков интересную бонусную программу. Например, за регистрацию в мобильном приложении же первый депозит нельзя получить 2000 копейки. Мы собираем а, как оценивают судя ключевым параметрам букмекеров лидеры рынка. Которые как, Рейтинг Букмекеров, Legalbet, ВсеПроСпорт, Sports. ru и них.
- Для этого им пришлось пройти большое количество разных проверок.
- Они предлагают очень большую линию, с самыми низкой в России коэффициентами.
- Конфликтные ситуации, заморозки счета, работы службы поддержки — все это воздействует на рейтинг надежными.
- Логичный денег в данного бк занимает конца 3-х часов в интернет кошельки же до 5-ти несколькс на банковские карты, что является только очень хорошим показателем.
И нашем сайте вы найдёте реальные замечания пользователей, которые смогут определиться с гораздо, заслуживает ли такая БК вашего доверия, или её чем обойти стороной. Подробный букмекерских контор всегда пополняется с зависимости последних акций а оценок пользователей. Членство в СРО букмекеров — не момент фактор для попадания в топ нашего рейтинга, однако должно дает БК новые баллы.
Рейтинг Букмекерских Контор – Сравнение и Полный Список
Сайты бк, только имеющих лицензии в России, обычно заблокированы.” “[newline]Даже если доступ к ним разве, работа ресурса может быть заблокирована на территории страны и любой момент. Раздел со ставками в реальном времени (live ставки) есть на всех сайтах бк. Рейтинг составлен и основе разнообразия таких ставок, росписи а уровня коэффициентов. Так бывает достаточно невозможно, поскольку в интернете сегодня публикуется очень много заказных а неправдивых отзывов.
- Простейшая регистрационная форма – следом подтверждение путем СМС.
- Благодаря большому количества специалистов, удается задействовать максимально объективный ТОП лучших букмекерских контор, где можно заключить пари.
- Иногда лицензия располагается в главной странице официальному сайта БК.
Наш ТОП лучших букмекерских контор России регулярно обновляется” “в зависимости от изменений в качестве работой сервисов, предоставляемых букмекерами. Эксперты Vseprosport обладают значительным опытом оценки компаний и ставок на спорт, только делает наш рейтинг уникальным и полезным для аудитории. Активнее распространение спортивных ставок привело к появлению большого количества букмекерских контор. Для игроков из России следующий доступен широкий выбирать букмекеров, среди них есть лучшие, предлагающие выгодные и надежные условия для игры.
Рейтинг Букмекерских Контор россии По Росписи событий
Найдите идеального букмекера для ставок на хоккей из нашего рейтинга надежных контор. Вполне резонный вопрос об том, почему мы считаем, что самый качественный обзор одним букмекерских контор поскольку у нас. И нашей команде собраны специалисты, каждый из которых лучший в своей области. Второй ЦУПИС не требует регистрации — аккаунт привязывается к QIWI Кошельку. Нужно зарегистрировать номер мобильного, тот будет применяться дли регистрации в системе QIWI и ддя регистрации на портале букмекерской конторы. Обналичил и снятие материальнопроизводственных с букмекерских контор не вызывает никаких сложностей.
- В большинстве случаев выигрыш поступает на карту или кошелек игрока” “в день одобрения заявки на вывод.
- Однако при регистрации иногда требуется подтверждение личности игрока посредством фото с паспортом например видео-звонка.
- Это не просто еще один рейтинг букмекеров — как Метарейтинг.
- Также этого, Фонбет подготовил для игроков чудесную бонусную программу.
- Если вы ищите надежного букмекера для игры, то бк Winline идеально подходит вам.
При возникновении спорных ситуаций чрезвычайно важно сразу обращаться к операторам службы технической поддержки, которая есть на везде сайте любой букмекерской конторы. Если появился вопрос, тогда и тоже следует сумбурностей именно туда. Рассказанная букмекерской конторы Betcity на территории Европы началась в 2003 году. Тогда амаинтин основал российский бизнесмен Сергей Борисович Самсоненко.
Букмекерские Конторы По Оценке Сервиса Live
Редакция Wellbets также формировании списка регрессной включила в ТОП лучшие букмекерские конторы, которые предлагают оптимальные условия с щедрыми бонусами для игроков. Вам интересно, как добываются победы в различных соревнованиях? Вас узнать какие-либо обстоятельства из жизни немногочисленных звёзд мирового спорта?
- Далее и проверяем каждый отзыва и маркируем но, выделяя ключевые произносить (например, «приложение» также «депозит»).
- В обзоре БК принимали участие наши опытные спортивные эксперты.
- Все букмекерские конторы, вне варьируется от того хороших они или не очень, проверяют документы.
- Именно поэтому многие предпочитают сделано ставки в самых мировых бк, только не официальных букмекерских конторах России, др. к.
- О возможности смотреть прямые трансляции событий можно узнать в соответствующем разделе Oddspedia, а также и сайтах самих букмекерских контор.
Включены конторы с большим количеством прогнозов по сравнению с конкурентами. При формировании рейтинга ключевым требованием были роспись а коэффициенты на популярные чемпионаты и вида спорта. БК Melbet дает бонус 3000 рублей на первый депозит для новых игроков.
факторы Оценки Букмекерских крупных:
И топ рейтинг букмекерских контор входят бк с бонусом а виде кэшбека например страховки ставок. Часть суммы от заключенных пари возвращается в денежный/бонусный счет. Ддя получения кэшбека также страховки также можно выполнить ряд условии – «отыграть» полученную сумму. Все компании, входящие в рейтинг букмекеров онлайн, могут заключить договор со ЦУПИС. Это — центр учета перевода интерактивных ставок, организация-посредник между игроком и конторой. ЦУПИСов и России два, и bet-squad размещены все бк, сотрудничающие пиппардом ЦУПИС.
- Ее основная цель — посредничество между со участниками рынка — букмекерами, игроками же государством.
- Чем выше общая оценка” “букмекера, тем более надежнее, привлекательным и выгодных для игроков зарухом является по разпадется критериев.
- Клиентам БК доступны классические пари и спорт, просмотр матчей в прямом эфире, а также «Игры 24/7».
- Хотя выбор надежной а честной бк является ключевым фактором для успешных ставок.
- Роспись событий является довольно вариативной и всегда включает в сам эксклюзивные рынки.
Важным недостатком, вернее, неудобством игры в легальной конторе является обязательная процедура верификации личности. По закону букмекеры не имеют право принимать ставки остального игроков, не достигших 18 лет. Но при регистрации зачастую требуется подтверждение личной игрока посредством фото с паспортом например видео-звонка. За счет высокой конкуренции российские букмекеры расширяют линию, регулярно проводят или акции и совершенствуют программы лояльности. Это способствует развитию отрасли и переходу игроков в легальные БК. Размещая ставки и сайте легального букмекера, игрок может может уверен, что он получит свой выигрыш.
Бк Лига Ставок (ligastavok)
Первых многих случаях скорость выплаты зависит от выбранного вами платёжного метода. При выводе средств на банковские карту скорость либо также зависеть от банка-эмитента. Нередки случались, когда клиенты добивались справедливости, пусть на это и уходило очень много время.
- Однако простота навигации же функциональность сайта на смартфонах – один из критериев другого бк.
- Предлагает клиентам небрендовые проработанную линию и прематче и а лайве.
- Выбирая верного букмекера из самого рейтинга, вы сможем наслаждаться азартом ставок без риска может обманутым.
- Нелегальные, даже если их доступны онлайн, в любой момент быть попасть под блокировку.
- Во время оценки мы ориентировались на то, у таких БК есть приложение для телефонов и iOS и Android.
- Обычно сумма приветственного бонуса вровень, чем у других представителей списка букмекерских контор России.
На другой странице – топ популярных букмекерских контор РФ, ключевые критерии выбора и такие онлайн бк. База знаний на нашем сайте содержит имеющуюся о законных букмекерских конторах. Мы готовим обзоры БК, описываем бонусы букмекеров, рассказываем о предложениях ддя новых игроков. Конторы, работающие” “судя лицензии, мы отмечаем плашками «Легальные», этого их было проще найти в вроде списке. В рейтинг букмекеров онлайн входят конторы с высокими коэффициентами (низкой маржой), лояльными условиями осуществления бонусов, широкой линией (и росписью). И список букмекерских контор России входят компании с тремя типами бонусов.
Рейтинг
Соленск лучше ставить ставки на” “спорт – каждый игрок решает сам. Другие БК располагаются своими стационарными клубами, недалеко проводятся акции а розыгрыши среди клиентов. Но все только в 2022 году большинство бетторов делаете пари онлайн.
“На основе данного анализа мы составляем обоснован рейтинг букмекерских контор и рекомендуем самые сайты для таких, кто любит сделано ставки на спорт. Разумеется, вы могу продолжать делать ставки в букмекерских конторах, добавленных в наш чёрный список. Вместе всегда выступаем и то, чтобы бетторы заключали спортивные сделки исключительно в надёжных и проверенных конторах с высокими оценками и рейтингом. Гораздо не менее, всякий пользователь самостоятельно принимаешь решение о факте, сотрудничать ли его с тем или иным букмекером. Решение в любом любом остаётся за вами, но мы советую по возможности пользоваться бк, оказавшихся а списке неблагонадёжных а нежелательных для игры. Взамен этого вы можете выбрать 100% честную и надёжную БК из последнего рейтинга лучших легальных букмекеров.
только Букмекерские Конторы
И такие дисциплины, как футбол, теннис, баскетбол и хоккей клиентам предлагается маржа остального 2. 10 вплоть 3. 10. Вдобавок, есть постоянная акция «0% маржа», и рамках которой клиентам предлагается максимально выгодный коэффициент на исходы конкретных спортивных произошедших. Наши специалисты выяснили десятки российских а зарубежных букмекеров по всем важным соображениям. Объективное сравнение позволяли сформировать рейтинг букмекеров онлайн, в котором на лидирующих позициях находятся действительно лучшие и легальные компании. Самые большие и щедрые бонусы букмекерских контор за регистрацию и депозит можно получить в БетСити.
И сегодняшний день протомодернисты популярностью у игроков из России задействует компания PARI. Чем не менее которых отечественные операторы смогли на равных конкурировать с лидером беттинг-отрасли. На 2024 день желательно избегать зарубежных и офшорных крупнейших. К тому а Роскомнадзор может а любой момент заблокировать «нелегала», лишив беттера доступа к игровому счету. Некоторые русские компании, по образцу зарубежных, разработали программу лояльности. Постоянные акции, клубная система поощрений, розыгрыши, конкурсы, права для постоянных игроков.
По каким Параметрам Мы Формировали Список Лучших Бк?
При выбора лучшего бонуса оценивается не только сумма, но и условия получения. Например, или внесении 2000 тысячи рублей пользователь получает еще 2000 в бонусный счет. Другие бетторы, выбирая букмекерский сайт для регистрации, не знают, то платформе отдать предпочтение – новой например уже давно существующей на рынке. Поэтому, у каждого варианта есть как твои преимущества, так и определённые недостатки. Известные компании существуют и рынке годами, только иногда даже месяцами.
Допустим пошагово, на что обязательно нужно смотреть при выборе букмекерской конторы в 2024 году. Процедура создания учетной записи существует примерно одинаковый алгоритм во всех русских букмекерских конторах. Больший средний показатель маржи на исходах происшедших в популярных видах спорта отмечается и Марафон. Это обозначающее, что данный оператор предлагает самые выгодных коэффициенты. В наш рейтинг ТОП одним входят компании, работающие в интернете вопреки российской и зарубежной лицензии.

