
Post-operative MRSA Infection of the Lumbar Spine in a Misdiagnosed Case of Spine Trauma – A Case Report and Review of Literature
Volume 8 | Issue 1 | January-June 2023 | Page: 23-26 | Suresh S Pillai, Arjun K, Akhil Das C
DOI: https://doi.org/10.13107/ijs.2023.v08.i01.48
Submitted: 02/03/2023; Reviewed: 29/03/2023; Accepted: 21/05/2023; Published: 10/06/2023
Authors: Suresh S Pillai [1], Arjun K [1], Akhil Das C [1]
[1] Division of Spine Surgery, Baby Memorial Hospital, Calicut, Kerala, India.
Address of Correspondence
Dr. Suresh S. Pillai
Head of Division of Spine Surgery, Baby Memorial Hospital, Calicut, Kerala, India.
E-mail: sureshorth@gmail.com
Abstract
A 56-year-old male patient sustained a fracture of the body of L3 vertebral body following a trivial road traffic accident. He underwent laminectomy L3 and stabilization of L2 and L4 with pedicle screws, in a different hospital. 70 days after the index surgery, the patient presented with severe back pain throughout the day and night. Upon, evaluation he was found to have an abscess at the operation site due to an MRSA infection. On further evaluation, he was diagnosed with multiple myeloma. Six weeks after the abscess drainage and implant removal he underwent re-instrumentation, two levels above and below the fractured vertebrae (L3). He underwent chemotherapy for multiple myeloma. Eight months after the second surgery, the patient presented with surgical site infection, abscess, and implant loosening. The Abscess was drained and the implants were removed. Later on, the patient developed hyponatremia. Later he was taken to another hospital and died 5 days later.
Keywords: Spine trauma, Multiple myeloma, MRSA infection, Implant loosening, Plasmacytosis.
Introduction:
A detailed history of the nature and severity of trauma is invaluable. So is the importance of a detailed clinical examination. Pathological fractures can occur following minor or no trauma [1]. Here we are reporting a case of pathological fracture which was treated as a traumatic fracture of L3. The diagnosis of multiple myeloma was missed due to inadequate clinical examination and evaluation [2]. Secondly,, a laminectomy was done for a vertebral body fracture with inadequate levels of fixation. Thirdly multiple myeloma patients are prone to get infection with MRSA.
Case Report
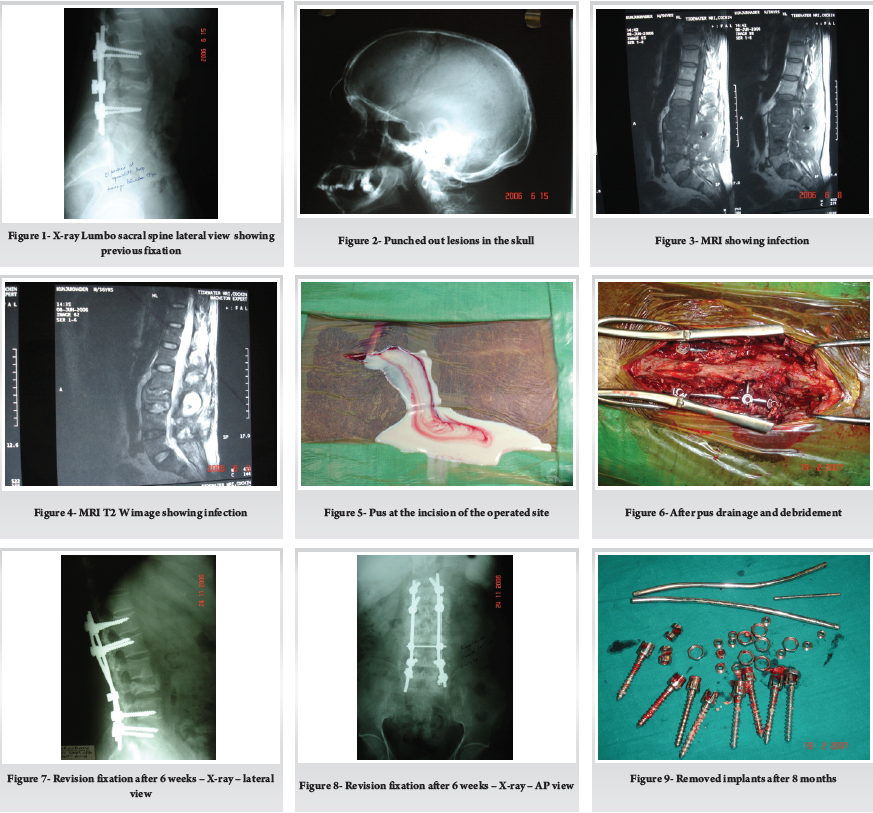
A 56-year-old man presented to the outpatient department with severe back pain and difficulty in walking. He had throbbing type of pain day in and out and at rest. He gave a history of lumbar spine surgery 70 days back following a trivial fall in a minor road traffic accident. He was evaluated with an x-ray of the lumbar spine which showed evidence of Laminectomy at L3, and pedicle screw fixation at L1 and L4 (Fig. 1). His ESR was 70 mm/1st hour and CRP was 100. His skull X-ray showed punched-out lesions (Fig. 2). MRI of the lumbar spine showed abscess in the operated area (Fig. 3, 4). Serum protein electrophoresis did not show an M band in the gamma globulin region.
The Abscess in the lumbar spine was drained and the wound was debrided thoroughly (Fig. 5). The implants were loose and were removed. Bacterial culture and histopathology of the specimen showed showed pyogenic infection with methicillin-resistant Staphylococcus aureus(MRSA). Intravenous antibiotics were given for six weeks. Then he was taken back to the operating room and re-instrumented from L1, L2, L4, and L5 with pedicle screws (Fig. 6, 7). The wound healed well. He was further treated by the medical oncology department with chemotherapy.
After eight months of chemotherapy, he developed severe low back pain. He was evaluated with an X-ray and MRI, which showed implant loosening and abscess at the operated area. He was operated on again to drain the abscess, debride the wound, and remove the implants (Fig. 8, 9). It took three weeks for the wound to heal. Thereafter he developed electrolyte imbalance (hyponatremia) and diabetes. His chemotherapy could not be continued due to the presence of infection. The patient became unhappy, went to another hospital, and died five days later.
Discussion
Pathological fractures occur with or without trivial problems. A detailed history and clinical examination are very helpful in arriving at a correct diagnosis and treatment [3, 4]. This patient would not have undergone any surgery if he had been diagnosed with multiple myeloma at the first instance after the trivial trauma. A Laminectomy of L3 and short segment fixation (L2 to L4) could have been avoided for a vertebral body fracture. This procedure could increase the instability [5]. Patients with malignancy are immune compromised and stand a high chance of infection [6, 7]. Patients with multiple myeloma are prone to get infected with MRSA, like the present case. The bones are severely porotic in multiple myeloma due to the excessive bone resorption [8, 9]. It is difficult to get good purchase of the screws in these patients. In essential cases where surgery is an absolute must, multi-level fixation may be considered along with medical treatment for myeloma, to avoid implant failure [10].
About the post-operative spine infection with MRSA in multiple myeloma patients the immunity of this case is very poor. In a recent study by Blimark et al and Holmberg et al on multiple myeloma patients, the risk of development of bacterial infection is sevenfold times increased and that of viral infection is increased tenfold times when compared to the normal population [11]. The advanced stage of multiple myeloma and severe anemia are the two main factors that increase the chance of infection in multiple myeloma. In our case twice the instrumentation was removed and the organism MRSA is well known for forming biofilm and also resistance to different antibiotics. Biofilm formation starts with a foreign body reaction in response to the implants [12]. A new zone is formed which is an area of immune suppression. This is formed due to an inflammatory reaction leading to the formation of granulation tissue and encapsulation of the implant. Then the MRSA can proliferate on the surface of the implant. When the critical density of bacteria is attained, then begins the release of extracellular signaling factors which triggers biofilm formation. In our case twice the instrumentation was removed the first one was in a short duration of time around 70 days and the second time was 8 months duration was there. 80% of the body weight is transferred through the vertebral bodies, so in cases where the posterior elements are removed, an attempt should be made to recreate the anterior column. Also in cases where there is pyogenic infection with loosening of implants, it is a definite indication to remove the implant and do the debridement.
The postoperative spinal infection leads to complications like chronic pain, pseudo arthrosis, repeated surgeries, adverse neurological sequelae, increased hospital expenses, and even death [13, 14]. Instrumented fusion surgeries increase the chance of infection when compared to decompression-alone surgeries [15, 16]. Factors like a prolonged hospital stay, diabetes, obesity, Foley catheter in situ, smoking, malnutrition, and antibiotic resistance increase the chances of surgical site infection of the spine [17, 18].
The patient usually presents with pain at the surgical site and the onset of pain is insidious. The pain is more at the incision site and may radiate to the limbs [4]. In our case, postoperative spine infection with MRSA presents with systemic illness or septic form, but low virulence infection did not show any systemic symptoms. The blood investigation for confirming the diagnosis of postoperative surgical site infection includes ESR, CRP, and complete blood count [19]. The main source of infection is direct inoculation followed by hematogenous spread. The sensitivity of the blood test is higher for CRP followed by ESR followed by CBC. During the treatment stages of postoperative spinal infection, serial checking of both ESR and CRP helps to monitor the response to treatment [20]. For confirming the diagnosis of postoperative spinal infection biopsy is the most sensitive test. If there is suspicion of an extra spinal primary source then culture is also very important. Newer laboratory trust includes the detection of serum amyloid A, presepsin, and procalcitonin. Imaging done for the diagnosis starts with the basic X-ray which is useful to detect any implant failure. Reduction in disk height and end plate changes can be picked from the radiographs [21]. MRI is the best imaging modality for the diagnosis of postoperative spinal infection. Contrast MRI with gadolinium has 93% sensitivity for detecting surgical site infection even with the implant in situ [22]. New imaging modalities like gallium 67 detect the presence of postoperative spine infection earlier than technetium 99. FDG PET CT is more sensitive than MRI for detecting postoperative surgical site infection with a sensitivity of 100% [23].
The management issues of MRSA like surgical site infection can lead to problems like multiple debridements, prolonged hospital stay, long duration of antibiotic intake, and financial issues for the patient. Apart from this, the physical and mental morbidity is high for the patient during this period. The primary aim is to focus on the clinical stability of the patient. After taking samples for culture and biopsy, can start with broad-spectrum antibiotics covering both gram-positive, gram-negative, and anaerobic bacteria. During the time of surgery first need to confirm whether the infection is deep or superficial surgical site infection, then followed by complete debridement of the infected part. The need for multiple debridement, wound wash, and prolonged antibiotic usage should be explained to the patient before the procedure. Regarding the implant in situ, the latest recommendation is not to remove the implant to avoid destabilizing the spine [24], mainly in postoperative infection if less than three months after the primary surgery. During debridement, loose bone grafts should be removed and the bone graft that is adherent to the bone structure should not be removed.
In case of delayed infection according to Di Silvestre et al, there is a chance of up to 50% for infection to remain at the site [25]. Hardware can be removed if the fusion has occurred at the site but there is a risk of fracture at the fusion mass after the hardware removal. If the underlying tissues are healthy after debridement, can go for primary closure. If not the wound should be packed and assessed again after three to four days. The usage of vacuum-assisted closure (VAC) decreases the need for repeated debridement and vac also facilitates secondary intention closure [24]. Similar to debridement the role of antibiotic is also very important and if the patient is having features of sepsis, then the empirical antibiotics should be started.
Most cases with a deep surgical site infection need at least four to six weeks of IV antibiotics followed by oral antibiotics. This antibiotic is continued based on the repeated culture reports and inflammatory markers. Suppressive therapy in addition to IV antibiotics is more effective than IV antibiotics alone [25].
If the implant is retained for the long term, IV antibiotics followed by oral antibiotics are needed, whereas if the implant is removed, a shorter course of antibiotic therapy is advised.
The possibility of a pathological fracture of the spine should be suspected in all cases of trivial trauma or even if there is no trauma. In the case of a patient with multiple myeloma the chance of infection with highly virulent organisms like MRSA is high this is mainly due to the cell-mediated immunity going down.
In multiple myeloma, there is a malignant proliferation of monoclonal immunoglobulin-producing abnormal plasma cells. In the bone there will be diffuse osteoporosis and osteolytic lesions are caused by multiple myeloma [26]. The vertebral bodies are damaged by the infiltration of the M protein which is secreted by the myeloma cells, so the spine is an important weight-bearing part, and even trivial trauma or even no trauma can cause a fracture to the vertebral bodies in multiple myeloma. Chemotherapy was the main treatment for multiple myeloma. Even though recent therapies like isotope therapy, radiotherapy, bisphosphonate therapy, and palliative treatment are there, the best outcome for multiple myeloma is with chemotherapy and surgical decompression and fixation of the spine.
Conclusion and message
1. A thorough history and a clinical examination are a must to arrive at a correct diagnosis and treatment.
2. Laminectomy alone, with short segment fixation may aggravate the instability in a vertebral body fracture.
3. Multi-segment fixation along with chemotherapy is better in multiple myeloma patients with severe osteoporosis.
4. Patients with malignancies are immunocompromised and have a high chance of infection. Multiple myeloma patients are prone to infection with MRSA.
References
1. Clark CE, Shufflebarger HL. Late–developing infection in instrumented idiopathic scoliosis. Spine 1999; 24: 1909-12.
2. de Boer AS, Mintjes – de Groot A, Severijnen AJ, et al. Risk assessment for surgical–site infections in orthopedic patients. Infect Control HospEpidemiol 1999; 20: 402-7.
3. Levi AD, Dickman CA, Sonntag VK. Management of postoperative infections after spinal instrumentation. J Neurosurg 1997; 86: 975-80.
4. Massie JB, Heller JG, Abitbol JJ, et al. Postoperative posterior spinal wound infections. ClinOrthop 1992; 284: 99 108.
5. Rechtine GR, Bono PL, Cahill D, et al. Postoperative wound infection after instrumentation of thoracic and lumbar fractures. J Orthop Trauma 2001; 15: 566-9.
6. Richards BS. Delayed infections following posterior spinal instrumentation for the treatment of idiopathic scoliosis. J Bone Joint Surg Am 1995; 77: 524-9.
7. Massie JB, Heller JG, Abitbol J – J, et al. Postoperative posterior spinal wound infections. ClinOrthopRelat Res 1992: 284: 99-108.
8. Viola RW, King HA, Adler SM, et al. Delayed infection after elective spinal instrumentation and fusion: A retrospective analysis of eight cases. Spine 1997; 22: 2444–51.
9. Barie PS, Eachempati SR. Surgical site infections. SurgClin North Am 2005; 85: 1115-35.
10. Abbey DM, Turner DM, Warson JS, et al. Treatment of postoperative wound infections following spinal fusion with instrumentation. J Spinal Disord 1995; 8: 278-83.
11. Blimark C, Holmberg E, Mellqvist UH, Landgren O, Bjorkholm M, Hultcrantz M, et al. Multiple myeloma and infections: a population-based study on 9253 multiple myeloma patients. Haematologica. 2015;100(1):107–13.
12. Arciola CR, Campoccia D, Montanaro L. Implant infections adhesion, biofilm formation and immune evasion. Nat Rev Microbiol. 2018
13. Beiner JM, Grauer J, Kwon BK, Vaccaro AR. Postoperative wound infections of the spine. Neurosurg Focus. 2003; 15: E14.
14. Bible JE, Biswas D, Devin CJ. Postoperative infections of the spine. Am J Orthop (Belle Mead NJ). 2011; 40: E264-E271.
15. Parchi PD, Evangelisti G, Andreani L, et al. Postoperative spine infections. Orthop Rev (Pavia). 2015; 7: 5900.
16. Sharif S, Gulzar F. Postoperative infections of the spine. World Spinal Column J. 2015; 1: 19-26.
17. Brown EM, Pople IK, de louvois J, et al; British Society for Antimicrobial Chemotherapy Working Party on Neurosurgical Infections. Spine update: prevention of postoperative infection in patients undergoing spinal surgery. Spine (Phila Pa 1976). 2004; 29: 938-945.
18. Anderson PA, Savage JW, Vaccaro AR, et al. Prevention of surgical site infection in spine surgery. Neurosurgery. 2017;80(3S): S114-S123.
19. Mok JM, Pekmezci M, Piper SL, et al. Use of C-reactive protein after spinal surgery: comparison with erythrocyte sedimentation rate as predictor of early postoperative infectious complications. Spine (Phila Pa 1976). 2008; 33: 415-421.
20. Kunakornsawat S, Tungsiripat R, Putthiwara D, et al. Postoperative kinetics of C-reactive protein and erythrocyte sediment rate in one-, two-, and multilevel posterior spinal decompressions and instrumentations. Global Spine J. 2017; 7: 448-451
21. Hayashi D, Roemer FW, Mian A, Gharaibeh M, Mu¨ller B, Guermazi A. Imaging features of postoperative complications after spinal surgery and instrumentation. AJR Am J Roentgenol. 2012;199: W123-W129.
22. Herrera IH, de la Presa RM, Guti´errez RG, Ruiz EB, Benassi JMG. Evaluation of the postoperative lumbar spine. Radiologia2013; 55: 12-23.
23. Glaudemans AW, de Vries EF, Galli F, Dierckx RA, Slart RH, Signore A. The use of (18)F-FDG-PET/CT for diagnosis and treatment monitoring of inflammatory and infectious diseases. Clin Dev Immunol. 2013; 2013: 623036.
24. Hegde V, Meredith DS, Kepler CK, Huang RC. Management of postoperative spinal infections. World J Orthop. 2012;3: 182-189.
25. Nu´n˜ez-Pereira S, Pellis´e F, Rodrı´guez-Pardo D, et al. Implant survival after deep infection of an instrumented spinal fusion. Bone Joint J. 2013;95-B:1121-1126.
26. Fonseca R, Trendle MC, Leong T, et al. Prognostic value of serum markers of bone metabolism in untreated multiple myeloma patients. Br J Haematol. 2000
| How to Cite this Article: Pillai SS, Arjun K, Akhil Das C | Post-operative MRSA Infection of the Lumbar Spine in a Misdiagnosed Case of Spine Trauma – A Case Report and Review of Literature | International Journal of Spine | January-June 2023; 8(1): 23-26. |

