
Osteoid Osteomas of Spine: From open to minimally invasive excision of the Nidus – A Case series
Volume 8 | Issue 1 | January-June 2023 | Page: 18-22 | S. Ganesh Kumar, Sudeep Kumar V.N, Sivakumar Raju, Vinoth Thangamani, Bharatkumar Ramalingam Jeyashankaran, Chidambaram Muthu
DOI: https://doi.org/10.13107/ijs.2023.v08.i01.47
Submitted: 10/01/2023; Reviewed: 23/01/2023; Accepted: 14/04/2023; Published: 10/06/2023
Authors: S. Ganesh Kumar [1], Sudeep Kumar V.N [1], Sivakumar Raju [1], Vinoth Thangamani [1], Bharatkumar Ramalingam Jeyashankaran [1], Chidambaram Muthu [1]
[1] Department of Spine Surgery, Preethi Hospitals, Melur Main Road, Uthangudi, Madurai, Tamil Nadu, India.
Address of Correspondence
Dr. S. Ganesh Kumar,
Post-Doctoral Fellow in Spine Surgery, Preethi Hospitals, Melur Main Road, Uthangudi, Madurai, Tamil Nadu, India.
E-mail: sgk.ortho@gmail.com
Abstract
Osteoid osteomas of spine are not uncommon and majority of which occurs in posterior elements of lumbar spine. Management of such lesions in spine ranges from open en bloc excision to percutaneous radiofrequency ablation. In this series, we have managed three cases of osteoid osteomas of spine, each managed differently from conventional open technique to minimally invasive method. All three cases underwent appropriate radiological investigations and followed by surgical excision of the lesion and histopathological analysis post-operatively. First case was managed with open excision of the lesion with conventional unilateral pedicle screw stabilisation. Second case, who underwent open excision of the lesion developed recurrence which was managed by re-excision without any further complications. Last case underwent microendoscopic quadrant tubular excision of the tumour with unilateral MISS with pedicle screws.
The technique of Microendoscopic quadrant tubular excision of posterior element benign tumour had advantages of small skin incision, less bleeding, clear macroscopic visualisation of the small tumour (enables complete excision of the nidus thus decreasing the recurrence), early mobilisation and shorter hospitalization with effective and complete excision of the tumour better than open method. Further, histological evidence of tumour will be available. The complete excision of nidus using microendoscopic tubular retractors with unilateral fixation in young age gives encouraging results. This case series is followed by review of literature highlighting the role of COX-2 inhibitors in osteoid osteoma, cause for scoliosis and neurological deficit in osteoid osteoma and management of osteoid osteomas of spine.
Keywords: Tumor, Osteoid osteoma, Minimally invasive, Dorsolumbar spine, Excision biopsy
Introduction:
Osteoid osteoma is a benign and solitary bone forming tumour, making 10% of benign tumours of bone [1]. 10% – 25% occurs in spine, with preponderance (70%-100%) to posterior elements of spine, for unknown reasons [1,2,3]. Of these, about 56% occurs in lumbar spine [4]. Treatment for osteoid osteoma aims at complete removal of the nidus to prevent recurrences. Recently, minimally invasive techniques have been commonly used for the treatment degenerative spine diseases. In this series, we report three cases of osteoid osteoma of spine, one of which is managed through minimally invasive technique using microendoscopic quadrant tubular retractors.
Materials and Methods:
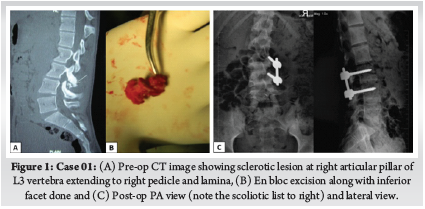
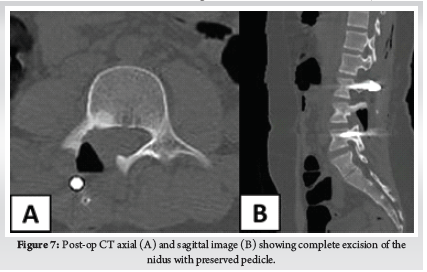
Our first case is a 15-year-old-boy, who had lower back pain (LBP) for 8 months with neither radicuolpathy nor signs of nerve irritation. Pain relieved by non-steroidal anti-inflammatory drugs (NSAIDS). Computed Tomography (CT) revealed a sclerotic lesion at right articular pillar of L3 vertebra extending to right pedicle and lamina with scoliotic list to right (Fig.1). He underwent open en bloc excision of the lesion and unilateral stabilisation with pedicle screws on L3-L4.
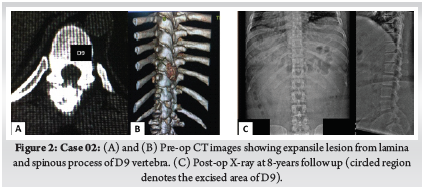
Second case, 36-year-old-male with pain in mid back region for 1 year duration, which has increased for last 15 days and not relieved by NSAIDS and also interfering with activities of his daily living. There was no symptoms or signs of nerve irritation. CT revealed a expansile lesion from lamina and spinous process of D9 vertebra with epidural soft tissue mass and new bone formation (Fig.2). He underwent open en bloc excision of the spinous process and right lamina. One year later, he developed recurrence, which was reoperated with wide local excision of the lesion. At 8-years follow up, no further recurrences noted.
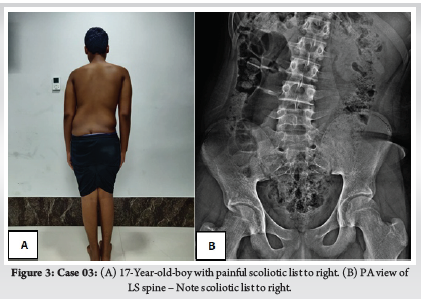
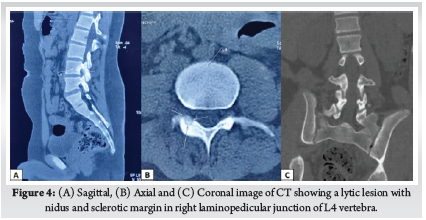
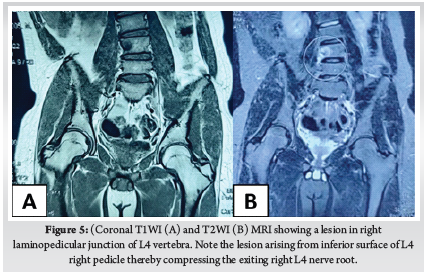
Third case is a 17-year-old-boy with LBP for 6 months of duration. At 2nd month of his symptom, he has undergone Magnetic Resonance Imaging (MRI), which was reported as normal study. He presented at 6th month of his symptom to our out-patient department (OPD) with persistent low back pain not relieved with NSAIDS and right lower limb radiculopathy with scoliotic list towards right (Fig. 3A). On examination there was weakness of right tibialis anterior with diminished sensation over right L4 dermatome. X-ray was taken which showed no obvious abnormality other than scoliotic list towards right (Fig. 3B). CT (Fig. 4) and MRI (Fig. 5) revealed a lytic lesion with nidus and sclerotic margin in right laminopedicular junction of L4 vertebra. Pre-operative Visual Analog Scale (VAS) for LBP was obtained. Excisional biopsy of the nidus with microendoscopic quadrant tubular retractors was performed. The details of all three cases are depicted in Table 1.
Surgical Technique:
The first and second case were operated through conventional open en bloc excision with addition of unilateral pedicle screw stabilisation for the former.
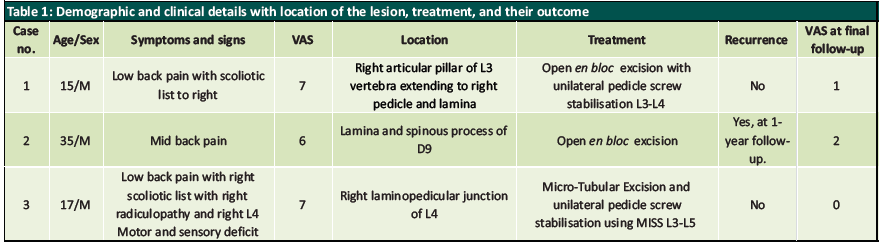
Third patient underwent excision of the nidus using microendoscopic quadrant tubular retractors. After positioning the patient in prone under general anaesthesia, fluoroscopy was performed intraoperatively before skin incision to know the exact location of insertion of quadrant tubular retractors. A 2cm skin incision was made 1.5 cm lateral to spinous process of L4 and after dorso-lumbar fasciotomy, the first dilator was docked at right spinolaminar junction of L4 vertebra. Then serial dilators (Medtronic Quadrant Tubular System) were inserted. Final dilator of size 22mm with 5mm depth was inserted and mounted to flexible arm attached to operating table (Fig. 6A). Right hemilaminectomy of L4 vertebra with facetal sparing was done. Then the nidus was reconfirmed under fluoroscopy and using microscope and burr, complete en bloc excision of nidus was done. The surrounding reactive tissues were also removed using rongeurs and curettes. After excision of the nidus, the exiting right L4 nerve root was found to be inflamed and oedematous (Fig. 6B). Then unilateral Minimally Invasive Surgical Stabilisation (MISS) with pedicle screws was done on ipsilateral pedicles of L3 and L5 vertebra (Fig. 6C). After haemostasis, wound closed with 3-0 ethilon. The patient was called for follow-up visits at regular intervals. Post-op VAS score was recorded. No complications were reported intra-operatively in all three cases. Histopathological Examination (HPE) of nidus of all three cases was done and were diagnostic of osteoid osteoma.
Results:
First case, recovered completely without any complications nor recurrence till 2-year follow-up. We have recommended implant removal after skeletal maturity, but for unknown reasons the patient lost his follow-up. Second case developed recurrence one year later and was reoperated with complete en bloc excision. No recurrences till 8-year follow-up with occasional pain only on intense activity.
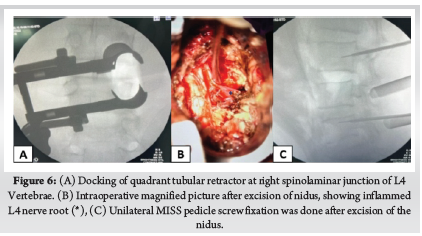
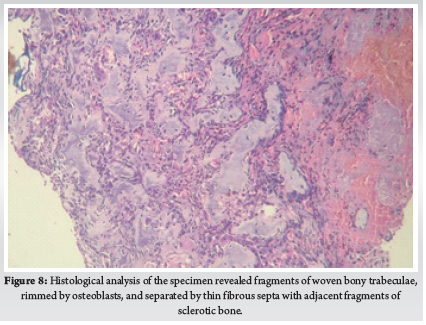
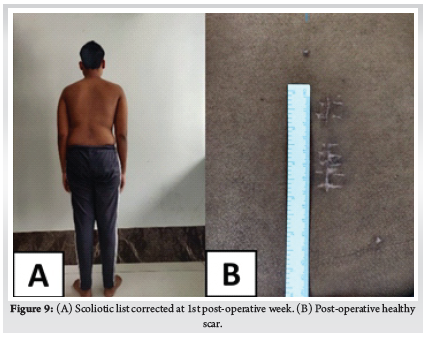
For the third case, the operative time was 90 minutes without significant blood loss. The radicular pain disappeared at once after surgery. The VAS score improved from 7/10 to 2/10 at immediate post-op period. The patient was made to walk on the evening of surgery and discharged on second post-operative day. Post-op CT showed the complete excision of the nidus with most of the pedicle kept intact (Fig. 7). HPE of the specimen (Fig. 8) confirmed our diagnosis. The scoliotic list resolved at first week (Fig. 9). The resolution of L4 neurological deficit occurred at sixth week. At second year follow-up visit, patient recovered completely without any complications nor recurrence.
Discussion:
Osteoid osteoma of spine is not an uncommon cause of LBP in adolescents presenting to ortho OPD. It is easily missed on first radiography due to its smaller size and complex anatomy of spine [5]. This is further complicated by highly variable appearance on MRI leading to its missed diagnosis [6]. This might be the reason our third case was initially missed, despite taking MRI initially. MRI may not clearly visualise the nidus and may only show peri-nidal marrow edema which might be confused with infection. CT scan is the most specific imaging modality in diagnosis of nidus [7]. A high level of cyclooxygenase-2 (COX-2) expression in neoplastic osteoblasts in the nidus of osteoid osteomas may cause the secondary changes depicted by MRI [8] and COX-2 is one of the important mediators of this condition [9] and this is the principle behind the use of NSAIDS in these lesions.
Almost two-third of osteoid osteoma of spine presents with painful scoliosis clinically [10]. Scoliosis in these patients is due to paravertebral muscle spasm and initially will be a non-structural one [11] later developing to a structural curve. A study by Ransford et al [12], reported that scoliosis persisted in patients who were operated after 15 months of symptoms. Delay in treatment might lead to persistence of scoliosis and becoming a structural one. So, the timing of treatment in those presenting with painful scoliosis is invaluable. In our series, two cases had scoliotic list, and both recovered after the excision of nidus. In both cases, the nidus was seen at concave side of the curve.
So far, no case of neurological deficit has been reported in the literature due to spinal osteoid osteoma [13]. Though spinal osteoid osteoma occurs close to neurological structures, deficit rarely occurs due to its small size [14]. Radiculopathy has been reported due to reactive inflammation caused by tumour [15]. In our series, first and second case had no symptoms or signs of nerve irritation. But third patient had right radiculopathy typically radiating along anterolateral aspect of thigh and medial aspect of leg with weakness of right ankle dorsiflexion and diminished sensation over medial malleolus. The neurological deficit in our case was due to reactive tissue arising from the inferior surface of L4 pedicle, which was compressing the right L4 nerve root as seen in pre-operative MRI (Fig. 5) .
The management of osteoid osteoma aims at complete excision or deactivation of the nidus to prevent the recurrences. Surgical excision is considered the optimal treatment modality for treating spinal osteoid osteoma [16]. The first and second case in our series was managed with open excision. One year after first surgery, second patient complained of pain at the same site, and was diagnosed with reactivation of lesion. Re-excision of the lesion was done and since the tumour was found at dorsal vertebra (D9), fixation was not done considering the inherent stability of dorsal vertebrae. The recurrence in this patient was due to incomplete excision of the lesion, which we think is a disadvantage of open excision due to difficulty in identifying the exact location of the lesion.
Radiofrequency ablation (RFA) is ideal choice if the nidus is located away from vital structures such as spinal cord, nerve roots and arteries. Rosenthal et. al [17, 18] who were the early pioneers of this method, suggested that the thermal necrosis was less safe if neural tissues were within 13 mm of the probe. Further, thin cortical bone of spine is not a reliable heat insulator and so percutaneous RFA for osteoid osteomas of spine carries a risk of neural damage [19]. Another disadvantage is histological evidence of osteoid osteoma is impossible with RFA. In our third case, the nidus was in such a location, where surgical excision would cause gross instability and RFA will be inappropriate as it is close to the right L4 nerve root. So, the microendoscopic quadrant tubular excision of the nidus was done with unilateral MISS pedicle screws on the same side pedicles of L3 and L5. This technique enables the magnified image of the nidus and its surrounding structures, which decreases the unnecessary wide bone resection, inadvertent injury to nerve roots and incomplete excision of the nidus as happened with our second case which resulted in recurrence of the tumour at 1-year.
Since, osteoid osteomas of spine are most common at pars interarticularis, its excision might cause instability which needs posterior stabilisation. In our series, 2 of 3 cases had nidus at pars interarticularis region. We did unilateral pedicle screw fixation using conventional open technique in first case and using MISS technique in third case. Unilateral pedicle screw fixation has advantages of decrease in operative time, length of hospital stays and blood loss with similar biomechanical advantage to bilateral pedicle screw fixation [20, 21]. Recently, Yang et al. [22] through their biomechanical study using finite element model and calf lumbar model, concluded that unilateral pedicle screw fixation is considered a safe and reliable technique. However, unilateral pedicle screw fixation has a disadvantage of increased cage migration, which is not applicable to our cases.
In open excision, the large surgical incision and inexact location of the nidus leads to incomplete excision of the nidus, increased paraspinal muscle damage with increased blood loss and creates bone defects which may require bone grafting, increasing the discomfort and expense of the patient [23, 24]. A case report of microendoscopic excision of C2 osteoid osteoma showed the advantages of minimal morbidity, minimal postoperative pain with less analgesic dependence, and better cosmesis [25]. The technique of microendoscopic quadrant tubular excision of posterior element benign tumour had advantages of small skin incision, less bleeding, clear macroscopic visualisation of the small tumour (enables complete excision of the nidus thus decreasing the recurrence), early mobilisation and shorter hospitalization with effective and complete excision of the tumour better than open method. Further, histological evidence of tumour will be available. With the advent of minimally invasive techniques, lesions of posterior element of spine can be safely excised and has more advantages than conventional open techniques.
Conclusion:
Osteoid osteomas of spine are easily missed due to their benign nature and variable appearance in imaging. So, high index of suspicion is needed in adolescent patients with painful scoliosis. The microendoscopic techniques using quadrant tubular retractor is already widely used for degenerative spinal diseases such as disc herniation, stenosis and facet cysts, its extended indication, as reported in our series, represents the newest and perhaps the most promising treatment for complete resection of tumours of this type. Thus, complete excision of nidus using microendoscopic tubular retractors with unilateral fixation in young age gives encouraging results.
References
[1] Gasbarrini, A., Cappuccio, M., Bandiera, S., Amendola, L., van Urk, P., & Boriani, S. (2011). Osteoid osteoma of the mobile spine: Surgical outcomes in 81 patients. Spine, 36(24), 2089–2093. https://doi.org/10.1097/BRS.0b013e3181ffeb5e
[2] Greenspan, A. (2004). Orthopedic Imaging: A Practical Approach. Lippincott Williams & Wilkins.
[3] Jackson, R. P., Reckling, F. W., & Mants, F. A. (1977). Osteoid osteoma and osteoblastoma. Similar histologic lesions with different natural histories. Clinical Orthopaedics and Related Research, 128, 303–313.
[4] Raskas, D. S., Graziano, G. P., Herzenberg, J. E., Heidelberger, K. P., & Hensinger, R. N. (1992). Osteoid osteoma and osteoblastoma of the spine. Journal of Spinal Disorders, 5(2), 204–211. https://doi.org/10.1097/00002517-199206000-00010
[5] Gamba, J., Martinez, S., Apple, J., Harrelson, J., & Nunley, J. (1984). Computed tomography of axial skeletal osteoid osteomas. American Journal of Roentgenology, 142(4), 769–772. https://doi.org/10.2214/ajr.142.4.769
[6] Davies, M., Cassar-Pullicino, V. N., Davies, A. M., McCall, I. W., & Tyrrell, P. N. M. (2002). The diagnostic accuracy of MR imaging in osteoid osteoma. Skeletal Radiology, 31(10), 559–569. https://doi.org/10.1007/s00256-002-0546-4
[7] Hosalkar, H. S., Garg, S., Moroz, L., Pollack, A., & Dormans, J. P. (2005). The diagnostic accuracy of MRI versus CT imaging for osteoid osteoma in children. Clinical Orthopaedics and Related Research, 433, 171–177. https://doi.org/10.1097/01.blo.0000151426.55933.be
[8] Kawaguchi, Y., Hasegawa, T., Oka, S., Sato, C., Arima, N., & Norimatsu, H. (2001). Mechanism of intramedullary high intensity area on T2-weighted magnetic resonance imaging in osteoid osteoma: A possible role of COX-2 expression. Pathology International, 51(12), 933–937. https://doi.org/10.1046/j.1440-1827.2001.01305.x
[9] Mungo, D. V., Zhang, X., O’Keefe, R. J., Rosier, R. N., Puzas, J. E., & Schwarz, E. M. (2002). COX-1 and COX-2 expression in osteoid osteomas. Journal of Orthopaedic Research: Official Publication of the Orthopaedic Research Society, 20(1), 159–162. https://doi.org/10.1016/S0736-0266(01)00065-1
[10] Janin, Y., Epstein, J. A., Carras, R., & Khan, A. (1981). Osteoid osteomas and osteoblastomas of the spine. Neurosurgery, 8(1), 31–38. https://doi.org/10.1227/00006123-198101000-00007
[11] Keim, H. A., & Reina, E. G. (1975). Osteoid-osteoma as a cause of scoliosis. The Journal of Bone and Joint Surgery. American Volume, 57(2), 159–163.
[12] Ransford, A. O., Pozo, J. L., Hutton, P. A., & Kirwan, E. O. (1984). The behaviour pattern of the scoliosis associated with osteoid osteoma or osteoblastoma of the spine. The Journal of Bone and Joint Surgery. British Volume, 66(1), 16–20. https://doi.org/10.1302/0301-620X.66B1.6693471
[13] Gasbarrini, A., Cappuccio, M., Bandiera, S., Amendola, L., van Urk, P., & Boriani, S. (2011). Osteoid osteoma of the mobile spine: Surgical outcomes in 81 patients. Spine, 36(24), 2089–2093. https://doi.org/10.1097/BRS.0b013e3181ffeb5e
[14] Zenmyo, M., Yamamoto, T., Ishidou, Y., Komiya, S., & Ijiri, K. (2011). Osteoid osteoma near the intervertebral foramen may induce radiculopathy through tumorous inflammation. Diagnostic Pathology, 6, 10. https://doi.org/10.1186/1746-1596-6-10
[15] Tekaya, A. B., Moalla, M., Salah, M. B., Saidane, O., Tekaya, R., Hadhri, K., Mahmoud, I., & Adbelmoula, L. (2021). Spinal Osteoid Osteoma Revealed by Radiculopathy: Case Report and Literature Review. International Journal of Spine Surgery, 14(s4), S26–S32. https://doi.org/10.14444/7161
[16] Mallepally, A. R., Mahajan, R., Pacha, S., Rustagi, T., Marathe, N., & Chhabra, H. S. (2020). Spinal osteoid osteoma: Surgical resection and review of literature. Surgical Neurology International, 11, 308. https://doi.org/10.25259/SNI_510_2020
[17] Rosenthal, D. I., Hornicek, F. J., Torriani, M., Gebhardt, M. C., & Mankin, H. J. (2003). Osteoid osteoma: Percutaneous treatment with radiofrequency energy. Radiology, 229(1), 171–175. https://doi.org/10.1148/radiol.2291021053
[18] Rosenthal, D. I., Springfield, D. S., Gebhardt, M. C., Rosenberg, A. E., & Mankin, H. J. (1995). Osteoid osteoma: Percutaneous radio-frequency ablation. Radiology, 197(2), 451–454. https://doi.org/10.1148/radiology.197.2.7480692
[19] Rybak, L. D., Gangi, A., Buy, X., La Rocca Vieira, R., & Wittig, J. (2010). Thermal ablation of spinal osteoid osteomas close to neural elements: Technical considerations. AJR. American Journal of Roentgenology, 195(4), W293-298. https://doi.org/10.2214/AJR.10.4192
[20] Lychagin, A., Cherepanov, V., Lipina, M., & Vyazankin, I. (2021). Comparison of the Unilateral and the Bilateral Pedicle Screw Fixation without Using an Interbody Cage: Randomized Clinical Trial. Open Access Macedonian Journal of Medical Sciences, 9(B), 398–402. https://doi.org/10.3889/oamjms.2021.6151
[21] Zhao, Y., Yang, S., & Ding, W. (2019). Unilateral versus bilateral pedicle screw fixation in lumbar fusion: A systematic review of overlapping meta-analyses. PloS One, 14(12), e0226848. https://doi.org/10.1371/journal.pone.0226848
[22] Yang, S., Xia, H., Cong, M., Guo, A., Ma, K., & Song, M. (2022). Unilateral pedicle screw fixation of lumber spine: A safe internal fixation method. Heliyon, 8, e11621. https://doi.org/10.1016/j.heliyon.2022.e11621
[23] Boscainos, P. J., Cousins, G. R., Kulshreshtha, R., Oliver, T. B., & Papagelopoulos, P. J. (2013). Osteoid osteoma. Orthopedics, 36(10), 792–800. https://doi.org/10.3928/01477447-20130920-10
[24] Çakar, M., Esenyel, C. Z., Seyran, M., Tekin, A. Ç., Adaş, M., Bayraktar, M. K., & Coşkun, Ü. (2015). Osteoid Osteoma Treated with Radiofrequency Ablation. Advances in Orthopedics, 2015, 807274. https://doi.org/10.1155/2015/807274
[25] Kulkarni, A. G., Dhruv, A. N., & Bassi, A. J. (2013). Microendoscopic excision of C2 osteoid osteoma: A technical report. Spine, 38(19), E1231-1234. https://doi.org/10.1097/BRS.0b013e31829cbf5e
| How to Cite this Article: Kumar SG, Sudeep Kumar VN, Raju S, Thangamani V, Jeyashankaran BR, Muthu C | Osteoid Osteomas of Spine: From Open to Minimally Invasive Excision of the Nidus – A Case series International Journal | of Spine | January-June 2023; 8(1): 18-22. |

