
Efficacy of Transforaminal Steroid Block for Pain Relief Due to Recurrent Lumbar Disc Herniation in Previously Operated Case of lumbar Discectomy
Volume 8 | Issue 1 | January-June 2023 | Page: 01-06 | Chandrasen Chaughule, Nitin Bhalerao, Anjaney Karangutkar, Jay Date, Sanket Tanpure, Srishti Tiwari
DOI: https://doi.org/10.13107/ijs.2023.v08.i01.44
Authors: Chandrasen Chaughule [1], Nitin Bhalerao [1], Anjaney Karangutkar [1], Jay Date [1], Sanket Tanpure [1], Srishti Tiwari [2]
[1] Department of Orthopaedics, Dr. Vikhe Patil Medical College, Ahmednagar, Maharashtra, India.
[2] Department of Anaesthesia, Dr. Vikhe Patil Medical College, Ahmednagar, Maharashtra, India.
Address of Correspondence
Dr. Chandrasen Chaughule,
Assistant Professor, Department of Orthopaedics, Dr. Vikhe Patil Medical College, Ahmednagar, Maharashtra, India.
E-mail: csfever10@gmail.com
Abstract
Background: lower Back discomfort as a result of a herniated disc is quite prevalent worldwide, frequently resulting in missed work days and significant changes in affect and motivation. Recurrent lumbar disc herniation is one of the most common problem faced after a lumbar discectomy, most frequently seen among male gender, tall-heighted individuals, heavy workers, obese and smokers. Analgesic and anti-inflammatory medication is the initial course of treatment. But in the majority of instances, it progresses slowly and calls for surgical intervention or minimally invasive treatments like steroid injections.
Aims and Objectives: The purpose of this study is to determine whether transforaminal steroid block can be attempted before surgery for pain relief in cases of recurrent herniated lumbar disc with failed conservative management having intractable radicular pain.
Materials & Methods: Use of transforaminal selective nerve root block (SNRB) in single level recurrent lumbar disc herniation patients was studied. 40 patients with single lumbar disc herniation, operated with discectomy were studied irrespective of age and sex. All patients were injected with a combination of long acting steroid suspension with local anaesthetic (Bupivacaine-plain) near the affected nerve root via cambins triangle approach and the results were analysed.
Result: Those graded mild, were pain free for up to an average of 5.5 months and those graded moderate had 3.3 months of relief. Patients suffering from extensive disc prolapse had immediate post procedural relief but not in long term. 47.5% patients have had a pain free interval upto 6 months.
Conclusion: Transforaminal SNRB is an excellent alternative for pain relief in patients with recurrent lumbar disc herniation having failed conservative management with intractable lumbar radicular pain. It was also found to be a cost effective alternative and relatively less invasive, with almost no complication.
Keywords: Selective nerve root block, Disc prolapse, Recurrent lumbar disc herniation.
Introduction
Recurrent lumbar disc herniation is defined as intervertebral disc herniation at the same level with a pain-free interval of more than six months, regardless of ipsilateral or contralateral herniation. There are several frequent pathologies of the spine, with a lifetime prevalence of 5–18%. In some circumstances, it resolves on its own or with the help of analgesic, anti-inflammatory, and physiotherapeutic therapy; nevertheless, it can also progress chronically with serious negative effects on the mind, society, economy, and quality of life. Transforaminal injections of small doses of steroids have lately been used to alleviate lower back pain, however the condition can become chronic and have severe negative effects on the quality of life. Recently, lower back discomfort brought on by a herniated disc has been successfully treated with transformational injection of modest quantities of steroids [1-6].
In both the cervical and lumbar areas, selective nerve root block (SNRB) is used to treat radicular pain brought on by a specific damaged nerve root [7-9]. Therapeutic efficacy needs to be discussed despite claims that it has a low degree of specificity as a diagnostic tool [10-11]. This modality is being used commonly for those with or without significant surgical spinal lesions [12]. Mechanical lesions include various stages of disc prolapse as in ligamentum flavum hypertrophy, facet hypertrophy and degenerative osteophytes causing foraminal stenosis, all leading to the nerve root irritation [13]. Transforaminal nerve root block has proven to be quite a specific procedure with excellent outcomes in cases of lumbar disc herniation. Being a pain-relieving interventional procedure, it also falls in the purview of different medical care specialists, including spine surgeons, radiologists, anaesthesiologists, and pain physicians, and thus the inclusion criteria and as a result, different studies have quite diverse inclusion requirements and patient evaluation standards. Patients in non-manual job (“white collared”) had a poor outcome with SNRB although studies have revealed a higher incidence of LDH in young, male patients engaged in severe manual labour, although the relationship between this finding and the results of LDH treatment is unclear. Significantly greater in patients with low work satisfaction and high stress employment, particularly those with jobs that required them to meet regular time-based deadlines. It has been demonstrated that obesity and a higher BMI are linked to recurrent LDH. Other risk factors are smoking, diabetes, etc. Another theory for the cause of the nerve root pain is an inflammatory reaction to an exposed nucleus pulpous [13]. The idea behind this method is to inject a steroid into the nerve root to minimise inflammation, which will lessen pain intensity. For their anti-inflammatory effects, these medications work through a variety of substrates by inhibiting phospholipase A2 which plays a significant role in the cascade and the pathophysiology of pain. Experimental models demonstrated that betamethasone might decrease the expression of substance P thus leading us to a possible role in pain mediating pathway. In addition, methylprednisolone has demonstrated effects leading to a decrease in edema and venous congestion with reduction of ischemia and pain. However, the actual disease causing the stimulation of the nerve roots is still unknown, thus recurrence is anticipated.
Our goal is to investigate the prognosis following a single dosage of SNRB over the damaged lumbar nerve roots to see its efficacy in reduction of pain in case of recurrent lumbar disc herniation.
Materials and methods
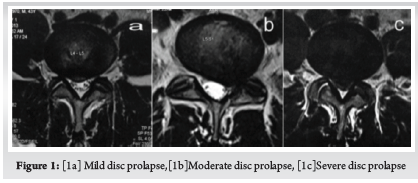
Patients were chosen based on different factors regardless of age and sex. Screening with MRI was done in all patients for identifying the lesion. Only those patients with intervertebral disc lesions affecting a particular lumbar nerve root, who were previously operated were selected for the study. Patients with more of back pain than radicular pain were to be excluded as a part of study also those having symptoms of bilateral and more than one nerve root involvement and those having neuro deficit. Patients’ MRI were graded according to MSU classification for herniated disc [14].
Inclusion criteria. : Patients previously operated for lumbar disc herniation (Endoscopic/ Microscopic) having a unilateral disc prolapse on same or the adjacent side or level, not responding to conservative modalities for more than 3 months and destined to have a revision surgery were included in study. (Fig. 1, 2)

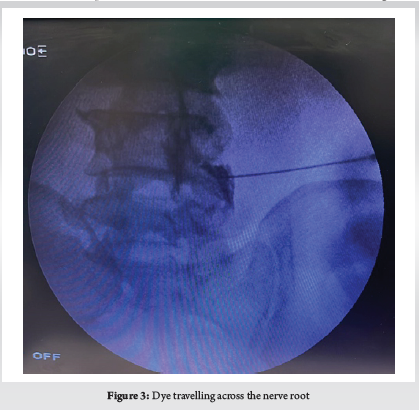
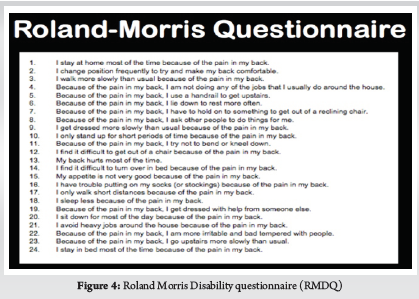
Before the operation, all patients completed the Roland Morris Disability Questionnaire (RMDQ) for back pain, and their results were recorded [15]. Numeric rating scale (NRS) for pain was used to grade pre-procedural pain on doing SLR [16]. Procedure took not more than 15 minutes. The patients which were selected had underwent a micro or open lumbar discectomy, followed by a conservative management plan that included rest and physical therapy but did not help the patients’ symptoms. Since there were no patients in our sample with pathology at any levels other than L4-L5 and L5-S1, L5 and S1 were our target nerve roots. No case of far lateral or foraminal disc prolapse were present, affecting l4 at L4-L5 or L5 at L5-S1. The procedure to direct L5 and S1 nerve root is different. (Fig. 3, 4)
Although there are discrepancies in the position of the C-arm and the direction of exposure change, this procedure is always done under C-Arm control. In the prone position, the patient’s lumbosacral spine is examined. The area has been set up and covered. An antero-posterior (AP) view of the lumbosacral junction is possible with the C-Arm in this posture. Identification of the L5 pedicle on that side in an AP C-Arm picture is required in order to target the damaged L5 nerve root. Normally, the L5 nerve leaves the body below and at the L5 pedicle. The L5 nerve usually exits just inferior to L5 pedicle. Adequate local anaesthetic was infiltrated under the skin 3–4 cm lateral to the inferior border of L5 pedicle where we usually enter. A 20-gauge spinal needle was introduced and directed to a point few millimetres below and lateral to the L5 pedicle where the nerve is usually found. If there is resistance by bony lamina, the needle is walked over the bony lamina to reach the desired point via kambin’s triangle approach. The first dorsal sacral foramen must be clearly visible in order to target the S1 nerve root, hence the C-Arm must be tilted perpendicular to the sacrum. Here the first dorsal foramen, where S1 leaves, is the intended location for the needle. We were very careful not to handle the needle aggressively. The patients were warned about the paraesthesia that would be felt along the path of their radicular pain when the needle would hit the nerve. This is done to stop the needle from injuring the nerve. (Table 1)
Sometimes, when it was difficult to induce paraesthesia, a lateral view was taken to validate the needle’s position. As soon as paraesthesia is elicited, needle is slightly withdrawn and 0.5 ml of an iodine based radiopaque dye is injected to confirm the position of needle [17]. Then a combination of 80 mg of triamcinolone-based suspension with local anaesthetic was injected over the affected nerve root. Post procedural paraesthesia due to local anaesthetic effect is expected. Numeric rating of pain using NRS on doing SLRT was used to analyse immediate effect of this procedure. The majority of patients were discharged on the same day of the treatment and advised to relax and refrain from strenuous activity for the first two days. They were instructed to check in after two days if their symptoms remained the same or one week later if they felt better. Patients were assessed with the Roland Morris Disability questionnaire for back pain, and their results were recorded every week also In the first month following the treatment and then monthly up to 6 months. Those with unchanged symptoms and recurrence went for a subsequent revision surgery and remaining patients were warned about recurrence of symptoms. (Fig. 4, 5)

Roland Morris Disability Questionnaire (RMDQ)
Result
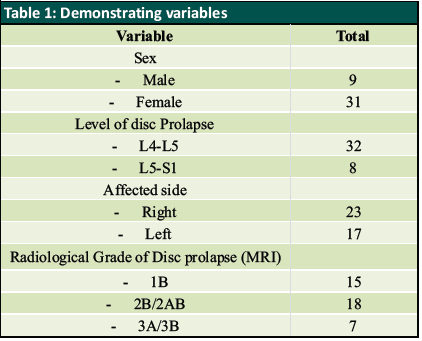
When performing straight leg raises on the afflicted side before the procedure, the mean NRS pain score was 8. The mean pre-procedure Roland Morris Disability questionnaire score was 23, and L5 nerve root was targeted in 32 patients (80%) who had L4 L5 intervertebral disc prolapse. L5 S1 disc prolapse affected 8 patients (20%), where S1 nerve root was involved. after the procedure on doing straight leg raising on the test on the involved side, the mean numbering rating of pain was reduced to 4 which was result of local anaesthetic effect. NRS assessment on doing SLR was done on 2nd day after the procedure for 4 patients who returned with similar pain. It was determined to be one point less or the same as pre procedure status. As per the protocol every patient was to be re-examined after one week and were given the Roland Morris Disability questionnaire for back pain and the score was recorded. At one week, the average RMDQ score was 10.35, which pointed to improvement. Revision surgery was suggested for those who experienced full recurrence in consecutive follow-ups and had RMDQ scores higher than 20. These patients were those who were deemed to be severe and in whom surgery was recommended but they were reluctant to go for surgery. After the first week, all of these patients experienced a near complete recurrence with an RMDQ score of 22 or above. They were informed of their unsatisfactory outcome further they all decided to have surgery. On excluding those 4 patients with recurrence our sample reduced to 36 patients (90%) with a mean RMDQ score of 8.1 by 2 weeks and 6.2 by 3 weeks. Review at one month had 5 patients with RMDQ scores more than 20. As a result they were omitted from study group and thus, reducing our sample size to 31 patients (77.5%). average RMDQ score of the revised study group was 7.8 by 1 month. Next follow up was by 2 months which had 6 patients with RMDQ scores more than 20. They were excluded and our group reduced to 25 patients (62.5%) with mean RMDQ score of 6.8. of the remaining sample size four patients started experiencing symptoms again at 3 months thus, reducing our group to 21 (52.5%). Mean RMDQ score of the remaining 21 was 9. By 4 months, 2 more patients had RMDQ score more than 20. Hence our group reduced to 19 patients (47.5%) with mean 4-month RMDQ score of 8.4. Thus, with a mean RMDQ score of 8.4 after 4 months, our cohort was decreased to 19 patients (47.5%). The average RMDQ score for these 19 patients at 5 months was 11.8; at 6 months, it was 13. After 6 months, patients with non-surgical radiological lesions were offered the option of receiving a second dose of SNRB, and all of them chose to do so. They were informed of our findings and prognosis.
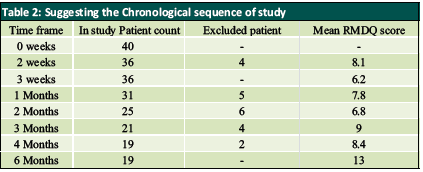
Analysing results showed that 90% patients had improvement by 2 weeks which reduced to 77.5% by 1 month (Table 2). Sequential follow-up showed a consistent decline in the number of patients reporting alleviation. By two months, only 62.5% of patients reported relief, which fell to 52.5% by three months and to 52.5% by four months. Finally, only 47.5% of patients were still pain free at six months, returning gradually to their pre-procedural condition. The final 47.5% of patients had a mild bulging disc to one side. According to our description based on MSU Classification, those graded mild had 5.5 months relief and that graded moderate had 3.3 months relief. Except for the immediate post-procedural relief, those with significant disc prolapse for whom surgery is recommended did not experience any relief.
Discussion
Lumbar radiculopathy secondary to a recurrent lumbar disc herniation is quite a challenging scenario in orthopaedic clinic. Patients who present with this complaints have an increasing trend. When treating these patients conservatively, results can vary greatly. The majority of patients who previously had a spine surgery initially reject surgery. Such people require a treatment that will at least temporarily reduce their agony. For these patients, SNRB is a critical treatment component. Also considering the morbidity and problems with revision lumbar spine surgery Transforaminal nerve root block has proved to be quite a specific procedure for pain relief with excellent outcomes in cases of recurrent lumbar disc herniation. Being a pain-relieving interventional procedure, it also falls in the purview of different medical care specialists, including spine surgeons, radiologists, anaesthesiologists, and pain physicians, and as a result the inclusion criteria and Patient evaluation differs greatly between trial. The prognosis for these people varies depending on the specific condition still causing the inflammation of the nerve root. Many authors have used methyl prednisolone-based preparations for this purpose [18]. Manchikanti et al demonstrated Transforaminal injections of local anaesthetic with or without steroids might be an effective therapy for patients with disc herniation. However present evidence illustrates the lack of superiority of steroids compared with local anesthetic at 2-year follow-up [22].
Patients with sedentary jobs fared poorly with SNRB. While studies have shown a higher incidence of Recurrent LDH in young, male patients engaging in heavy manual labour, their relationship with regard to the outcomes of LDH management has not been made clear. Studies have also shown that the incidence of LDH was significantly higher in patients who had high-stress jobs, particularly patients whose jobs required them to meet frequent time-based deadlines and patients with lower job satisfaction.
Morgan-Hough et al demonstrated, compared to extruded or sequestrated discs, a confined disc protrusion was almost three times more likely to require revision surgery. In comparison to patients with extruded or sequestrated discs, those with initial protrusions had a much higher straight leg rise and a lower prevalence of favorable neurological symptoms. Since these patients are three times more likely to need revision surgery, they should be excluded from care clinically and treated with a more zealous conservative approach emphasizing need for conservative management in lumbar disc herniations [23].
Study conducted by Kim J et al showed to have a comparison of nerve blocks and surgery that focused on radiological data, which was not previously proposed. According to the study’s findings, patients with disc herniations in the L4-5 that are longer than 6.31 mm may be candidates for surgery, whereas those with disc herniations less than 6.23 mm may benefit from nerve blocks. The threshold values for the radiological variables at 12 months exhibited nearly moderate discriminating power. However the study has limitations even if it is still promising. The study’s patient population was rather small, especially among the elderly, and it was retrospective in nature. Therefore, additional research involving more patients will be required before suggested cut-off values and may be used generally [24].
While performing the procedure the needle should not be handled roughly when the treatment is being performed because we only expect to lightly contact the nerve root. The majority of publications advice against doing this to avoid needle-induced problems, however none occurred in our study [17–20]. Using a quantitative pain rating scale, we assessed pain both before and after the procedure. Since focusing on the functional outcome was our main goal, we chose to employ the Roland Morris Disability Questionnaire. When the patient is unable to attend a follow-up appointment, this strategy can be helpful. according to questionnaire the severity of the prolapse was proportional to number of yes answers by the patient Based on the examination of serial questionnaire score 21, clinical improvement over time can be rated. Early response could not predict the effect after two weeks, as mentioned by a select few other writers. This quick relief may serve as a diagnostic tool to establish that the affected root is the obstructed root and has to be decompressed. It refers to how much relief the patient will get if that specific nerve root is surgically decompressed. Similar outcomes were obtained for those with mild and moderate prolapse, giving the majority of our patient’s time to consider their next course of treatment in case their pain reappears.
To the best of our knowledge, despite the lack of standardised guidelines, the goal of this study is to show how well steroid nerve root block works in treating recurrent lumbar disc herniation. Future large-scale randomised control studies should be conducted for a proper understanding
Conclusion
Numerous factors like tobacco chewing smoking, Lifestyle, obesity, intraoperative technique, and biomechanical factors may lead to occurrence of recurrent disc disease. Steroid nerve tansforaminal root block proved to be an excellent alternative for pain relief in patients with unilateral recurrent lumbar disc herniation, having failed conservative management complaining of intractable radicular pain with unilateral positive straight leg raise test. Considering the morbidity and complications as well as challenges with Revision Lumbar spine Surgery, It seemed a relatively less invasive with almost no complication. Although, the effect is typically unpredictable in its duration of course of pain free interval majority of patients yet it gains a valuable pain free interval in those patients with mild and moderate pathology. Also it proved to be a Cost effective, day care procedure with minimal morbidity with almost no complications.
References
1. Manson NA, McKeon MD, Abraham EP. Transforaminal epidural steroid injections prevent the need for surgery in patients with sciatica secondary to lumbar disc herniation: a retrospective case series. Can J Surg. 2013;56(2):89–96.
2. Collighan N, Gupta S. Epidural steroids. Contin Educ Anaesthe Crit Care Pain. 2010;10:1–5.
3. Vad VB, Bhat AL, Lutz GE, et al. Transforaminal epidural steroid injections in lumbosacral radiculopathy: a prospective randomized study. Spine. 2002;27(1):11–16.
4. Krych AJ, Richman D, Drakos M, et al. Epidural steroid injection for lumbar disc herniation in NFL athletes. Med Sci Sports Exerc. 2012; 44(2):193–198.
5. Baral BK, Shrestha RR, Shrestha AB, et al. Effectiveness of epidural steroid injection for the management of symptomatic herniated lumbar disc. Nepal Med Coll J. 2011;13(4):303–307.
6. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of Observational Studies in Epidemiology: A Proposal for Reporting. JAMA 2000;283(15):2008-2012.
7. Chung JY, Yim JH, Seo HY, Kim SK, Cho KJ. The Efficacy and Persistence of Selective Nerve Root Block under Fluoroscopic Guidance for Cervical Radiculopathy. Asian Spine J. 2012; 6: 227-32.
8. L Anderberg, M Annertz, L Persson, L Brandt, H Saveland. Transforaminal steroid injections for the treatment of cervical radiculopathy: a prospective and randomised study. Eur Spine J. 2007; 16: 321-8.
9. Narozny M, Zanetti M, Boos N. Therapeutic efficacy of selective nerveroot blocks in the treatment of lumbar radicular leg pain. Swiss Med Weekly 2001; 131: 75-80.
10. Beynon R, Hawkins J, Laing R, Higgins N, Whiting P, Jameson C, et al. The diagnostic utility andcost-effectiveness of selective nerve root blocks in patients considered for lumbar decompression surgery: a systematic review and economic model. Health Technol Assess 2013; 17(19).
11. Datta S, Manchikanti L, Falco FJ, Calodney AK, Atluri S, Benyamin RM, et al. Diagnostic Utility of Selective Nerve Root Blocks in the Diagnosis of Lumbosacral Radicular Pain: Systematic Review and Update of Current Evidence. Pain Physician 2013; 16(2 Suppl): SE97-124.
12. Epstein NE. The risks of epidural and transforaminal steroid injections in the Spine: Commentary and a comprehensive review of the literature. Surg Neurol Int 2013; 4: 74-93.
13. Stafford MA, Peng P, Hill DA. Sciatica: a review of history, epidemiology, pathogenesis, and the role of epidural steroid injection in management. Br J Anaesth. 2007; 99: 461-73.
14. Mysliwiec LW, Cholewicki J, Winkelpleck MD, Eis GP. MSU classification for herniated lumbar discs on MRI: Toward developing objective criteria for surgical selection. Eur Spine J 2010;19: 1087-1093.
15. Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine 1983; 8: 141-4.
16. Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011; 63: 240-252.
17. Pfirrmann CW, Oberholzer PA, Zanetti M, Boos N, Trudell DJ, Resnick D, et al. Selective nerve root blocks for the treatment of sciatica: evaluation of injection site and effectiveness–a study with patients and cadavers. Radiology. 2001 Dec; 221(3): 704-11.
18. Mobaleghi J, Allahdini F, Nasseri K, Ahsan B, Shami S, Faizi M, et al. Comparing the effects of epidural methylprednisolone acetate injected in patients with pain due to lumbar spinal stenosis or herniated disks: a prospective study. Int J Gen Med. 2011; 4: 875-8.
19. Blankenbaker DG, De Smet AA, Stanczak JD, Fine JP. Fine. Lumbar Radiculopathy: Treatment with Selective Lumbar Nerve Blocks- Comparison of Effectiveness of Triamcinolone and Betamethasone Injectable Suspensions. Radiology 2005; 237: 738- 41.
20. Slipman CW, Issac Z.. The Role of Diagnostic Selective Nerve Root Blocks in the Management of Spinal Pain. Pain Physician 2001; 4: 214-26.
21. M Roland, J Fairbank. The Roland Morris Disability Questioinaire and the Oswestry Disability Questionaire. Spine 2000; 25: 3115-24.
22. Manchikanti L, Cash KA, Pampati V, Falco FJ. Transforaminal epidural injections in chronic lumbar disc herniation: a randomized, double-blind, active-control trial. Pain Physician. 2014 Jul-Aug;17(4):E489-501.
23. Morgan-Hough CVJ, Jones PW, Eisenstein SM. Primary and revision lumbar discectomy. J Bone Joint Surg Br. 2003;85-B(6):871-874.
24. Kim J, Hur JW, Lee JB, Park JY. Surgery versus Nerve Blocks for Lumbar Disc Herniation : Quantitative Analysis of Radiological Factors as a Predictor for Successful Outcomes. J Korean Neurosurg Soc. 2016 Sep;59(5):478-84.
| How to Cite this Article: Chaughule C, Bhalerao N, Karangutkar A, Date J, Tanpure S, Tiwari S | Efficacy of Transforaminal Steroid Block for Pain Relief Due to Recurrent Lumbar Disc Herniation in Previously Operated Case of lumbar Discectomy | International Journal of Spine | January-June 2023; 8(1): 01-06. |

